Petition’s Provided To The NM Medical Cannabis Program in 2017, 2018, and 2019.
The New Mexico Department of Health will be holding two Medical Cannabis Advisory Board meetings: one on Monday, November 16, 2020, from 9:00 a.m. to 12:00 p.m. and one on Wednesday, December 9, 2020, from 9:00 a.m. to 12:00 p.m.
Jason Barker Albuquerque, NM 87109 SafeAccessNewMexico@gmail.com
Monday, November 11th 2019
(Petitions provided to NMDOH
Medical Cannabis Program Office
on November 12th 2019
via hand delivery)
New Mexico State Department of Health Medical Cannabis Advisory Board Medical Cannabis Program PO Box 26110 Santa Fe, NM, 87502-6110
Petition: Requesting The Inclusion Of A New Medical Treatment: Medical Cannabis Therapy For Seizures in Animals
( A medical cannabis card would be issued to a person as a qualified caregiver. Doctors of Veterinary Medicine are allowed to recommend under the current law’s requirement and the New Mexico Board of Veterinary Medicine allows DVM’s to discuss cannabis options. This Petitioned medical treatment is the missing link. )
There is no aspect of the current medical cannabis program laws that would prevent this new medical treatment for Medical Cannabis Therapy For Seizures in Animals from being approved into the Medical Cannabis Program. Doctors of Veterinary Medicine are qualifying medical professionals who can recommend medical cannabis.
Table of Contents Pg. 1 Cover Page Pg. 2 Table of Contents and Petition Background Pg. 3 - 13 Petition Narrative and Research Pg. 13-14 Petition Conclusion
Petition: Requesting The Inclusion Of A New Medical Treatment: Medical Cannabis Therapy For Seizures in Animals
( A medical cannabis card would be issued to a person as a qualified caregiver. Doctors of Veterinary Medicine are allowed to recommend under the current law’s requirement and the New Mexico Board of Veterinary Medicine allows DVM’s to discuss cannabis options. This Petitioned medical treatment is the missing link. )
The purpose of this Petition Requesting The Inclusion of a New Medical Treatment: Medical Cannabis Therapy For Seizures in Animals. And there is no aspect of the current medical cannabis program laws that would prevent this new medical treatment for Medical Cannabis Therapy For Seizures in Animals from being approved into the Medical Cannabis Program. Doctors of Veterinary Medicine are qualifying medical professionals who can recommend medical cannabis.
The use of cannabis as medicine for animals has been getting a lot of attention in the medical, scientific, and pet owning communities. One of the potential uses showing the most promise is in the treatment of seizures. And many of these animals have already been the research subjects enable current qualifying medical conditions in the medical cannabis program today. Ultimately there has been more cannabis research already tested on animals than compared to humans.
Meet Tecumseh, he’s my dog and 5 years old and he has the canine version of dravet syndrome - a rare, catastrophic, lifelong form of epilepsy.
The intent of Safe Access New Mexico is to establish The Inclusion of a New Medical Treatment: Medical Cannabis Therapy For Seizures in Animals for Veterinary Medical Cannabis access to the states Medical Cannabis Program to:
(a) Prevent the potential danger of animal abuse by regulating the use of medicinal cannabis on animals. (b) Give veterinarians the tools they need to treat their patients effectively without the fear of jeopardizing their license. (c) Ensure that access is readily available to animal patients. (d) Further research and knowledge throughout the health care system and for health care practitioners regarding medicinal cannabis.
The use of cannabis to treat seizures is nothing new. Cannabis has been described as a therapy for people with seizures for hundreds, if not thousands, of years. 1, 2
In recent years, cannabis, and cannabidiol (CBD) in particular, are once again being considered for the treatment of seizures in both humans and animals.
In ancient times, cannabis was used for seizures based purely on observational data, but today in-depth scientific research is being conducted to determine how and why cannabis is beneficial in the effort to determine how best to limit, and hopefully eliminate, seizures.
THE SCIENCE OF CANNABIS AND EPILEPSY Despite the renewed interest and availability for research funding, the mechanisms by which cannabis effects seizures are still unclear. One consideration is a specific receptor on neurons, known as “GPR55,” which is thought to mediate seizure activity through regulating the excitability of neurons. CBD appears to limit GPR55’s ability to cause neuronal excitation which is speculated to reduce seizures.
Additionally, somestudies have shown epileptic patients to have reduced anandamide (AEA) concentrations in their cerebrospinal fluid and/or alterations in their CB1 receptors. AEA is one of the naturally occurring neurotransmitters in the body that regulates the endocannabinoid system (ECS). CB1 receptors, also part of the ECS, are binding sites for AEA and changes in AEA and/or CB1 receptors are presumed to lead to changes in levels of other neurotransmitters that may ultimately lead to seizure activity. Tetrahydrocannabinol (THC) binds CB1 receptors and, in this way, may reduce seizure activity. 3, 4
The FDA-approved pharmaceutical Epidiolex is a single-molecule CBD formulation used to treat two forms of pediatric epilepsy.
Pre-clinical research into other cannabinoids and terpenes suggest other compounds found in cannabis may also be effective for seizure treatment. For practical and legal reasons, however, much of the current research focuses on CBD.
Although the exact reasons why cannabis compounds have a positive effect on seizures are not crystal clear, great strides have been made with regards to their therapeutic use.
In 2018, the FDA approved the first cannabis-derived pharmaceutical, Epidiolex. A single-molecule CBD formulation, Epidiolex is approved for the use of refractory seizures in two forms of pediatric epilepsy known as Lennox-Gastaut and Dravet Syndromes. Not only is Epidiolex of great benefit for the children it helps, the drug also represents a huge step forward in the federal government’s acknowledgement of the medicinal value of cannabis.
HOW DOES THE SCIENCE RELATE TO ANIMALS? Veterinary specific research has also taken a big step forward this year with the publishing of the first clinical trial evaluating the effects of CBD on seizures in epileptic dogs. The study, conducted at Colorado State University, evaluated seizure frequency in dogs with and without the use of CBD. Results showed an 89% reduction in seizure frequency in dogs who received 2.5 mg/kg CBD twice daily compared to a 43% reduction in dogs not receiving CBD. Both groups of dogs were receiving other anti-seizure pharmaceuticals at the time of the study which is the reason the group not receiving CBD had a large reduction in seizures, as well. While these results are considered statistically significant, they are certainly not as dramatic as many hoped they would be. The authors noted this in their conclusions and stated further studies are warranted to see if higher doses of CBD may be more beneficial in the treatment of seizures in dogs. 5
Dogs who received 2.5 mg/kg CBD twice daily experienced an 89% reduction in seizure frequency.
One specific point to note about the study is the CBD formula used was not a CBD “isolate.” The hemp-based formula contained “trace amounts of other cannabinoids” which may or may not have contributed to its efficacy. Research suggests that multiple cannabinoids (CBD, THC, and others) as well as terpenes have anti-seizure properties and it may be that greater effects can be found with a “broader spectrum” formulation.
Speaking from the perspective of the benefits of “whole plant medicine,” broad spectrum formulations are usually more effective than single components. That said, from a research perspective, using pure CBD would clarify what effects are specific to the one compound.
Anecdotal reports from pet owners and veterinarians suggest that cannabis can not only reduce seizure frequency, it may be able to lessen seizure severity, shorten recovery time, and potentially even prevent an imminent seizure if the animal is medicated at the first signs of trouble.
With research ongoing, we certainly see promise in the use of CBD, and potentially other cannabinoids, for the treatment of seizures in animals. That said, cannabis as medicine should be used with caution. CBD given at moderate to high doses can potentially effect blood levels of other medications, including anti-seizure drugs. Because of this, it may be necessary to monitor levels at the beginning of cannabis therapy. For the safety of your furry family members, always consult with your veterinarian before starting any form of cannabis therapy for your pet. BY Gary Richter on October 30, 2019 For ProjectCBD
Gary Richter, MS, DVM, CVA, CVC, GDWVHM, a Project CBD contributing writer, is an Oakland-based veterinarian. His articles focus on practical information for using cannabis to treat medical conditions in pets.
FOOTNOTES
Zaheer S, Kumar D, Khan MT, Giyanwani PR, Kiran F. Epilepsy and Cannabis: A Literature Review. Cureus. 2018;10(9).
Alison Mack; Janet Joy. Marijuana As Medicine?: The Science Beyond the Controversy. 2000; National Academies Press.
Perucca E. Cannabinoids in the Treatment of Epilepsy: Hard Evidence at Last?. J Epilepsy Res. 2017;7(2):61–76.
Bazelot, M, Whalley, B, Investigating the Involvement of GPR55 Signaling in the Antiepileptic Effects of Cannabidiol. Neurology. 2016, 86 (16 Supplement)
McGrath S, Bartner LR, Rao S, Gustafson DL. Randomized blinded controlled clinical trial to assess the effect of oral cannabidiol administration in addition to conventional antiepileptic treatment on seizure frequency in dogs with intractable idiopathic epilepsy. J Am Vet Med Assoc. 2019 ;254(11):1301-1308.
Research: Colorado State University’s College of Veterinary Medicine and Biomedical Sciences took the lead in veterinary CBD research in 2016. Dr. Stephanie McGrath and her team at CSU investigated the safety of specified combinations and delivery methods of our hemp-hybrid oil extract in dogs. The results confirmed that dogs tolerated clinical doses of the cannabis oil. These results were presented at the Institute of Cannabis Research Conference at CSU-Pueblo on April 29, 2017, and were published in the Fall 2018 issue of the Journal of the American Holistic Veterinary Medical Association.
Phase 2 Clinical Trials for Epilepsy and Arthritis Dr. McGrath completed a pilot epilepsy study in 2018, and the promising results of that study were published in the June 1 issue of the Journal of the American Veterinary Medical Association. A larger epilepsy study, sponsored by the AKC Canine Health Foundation, is ongoing at CSU, as is an arthritis study.
Randomized blinded controlled clinical trial to assess the effect of oral cannabidiol administration in addition to conventional antiepileptic treatment on seizure frequency in dogs with intractable idiopathic epilepsy. McGrath S, Bartner LR, Rao S, Packer RA, Gustafson DL.
Abstract OBJECTIVE: To assess the effect of oral cannabidiol (CBD) administration in addition to conventional antiepileptic treatment on seizure frequency in dogs with idiopathic epilepsy.
ANIMALS: 26 client-owned dogs with intractable idiopathic epilepsy.
PROCEDURES: Dogs were randomly assigned to a CBD (n = 12) or placebo (14) group. The CBD group received CBD-infused oil (2.5 mg/kg [1.1 mg/lb], PO) twice daily for 12 weeks in addition to existing antiepileptic treatments, and the placebo group received noninfused oil under the same conditions. Seizure activity, adverse effects, and plasma CBD concentrations were compared between groups.
RESULTS: 2 dogs in the CBD group developed ataxia and were withdrawn from the study. After other exclusions, 9 dogs in the CBD group and 7 in the placebo group were included in the analysis. Dogs in the CBD group had a significant (median change, 33%) reduction in seizure frequency, compared with the placebo group. However, the proportion of dogs considered responders to treatment (≥ 50% decrease in seizure activity) was similar between groups. Plasma CBD concentrations were correlated with reduction in seizure frequency. Dogs in the CBD group had a significant increase in serum alkaline phosphatase activity. No adverse behavioral effects were reported by owners.
CONCLUSIONS AND CLINICAL RELEVANCE: Although a significant reduction in seizure frequency was achieved for dogs in the CBD group, the proportion of responders was similar between groups. Given the correlation between plasma CBD concentration and seizure frequency, additional research is warranted to determine whether a higher dosage of CBD would be effective in reducing seizure activity by ≥ 50%. [https://www.ncbi.nlm.nih.gov/pubmed/31067185]
The CBD clinical safety and efficacy trials at CSU are highlighted in the recently published Nutraceuticals in Veterinary Medicine textbook. With over sixty chapters covering supplements and their use in animals, this textbook from Springer is a comprehensive resource for veterinarians and researchers. Chapter 10—entitled “Cannabis in Veterinary Medicine: Cannabinoid Therapies for Animals—delves deep in the science and research around veterinary use of cannabis and CBD.
Comprehensive Treatment of Veterinary CBD Use The chapter covers everything from the history of veterinary cannabis use and regulatory and legal considerations to a deep dive into the chemistry of the cannabis plant and the pharmacology of cannabinoids such as cannabidiol (CBD).
Highlighted topics include:
The 2018 Farm Bill and its effects on industry and research
Detailed look at the endocannabinoid system (including a terrific graphic illustrating the feedback loop for the endocannabinoid signaling system)
Nutritional value of Cannabis/Hemp seed oil – Fatty acid profile has anti-inflammatory properties
Review of the endocannabinoid system (ECS) in humans – including beneficial effects for sleep, anxiety and stress, obesity and metabolic disorders, cancer, and inflammatory conditions
Review of the ECS in animals – focuses on dogs but touches on all mammals, birds, fish, and even invertebrates
Phytocannabinoids, terpenes, and the Entourage effect (importance of full spectrum CBD product to achieve synergistic benefits from all compounds)
Good manufacturing processes and the importance of organic hemp
The importance of third party lab testing for potency and contamination
Completed and ongoing clinical trials at Colorado State University and Cornell
Reference: Frances R. Sowers, Executive Director of the New Mexico Board of Veterinary Medicine director@nmbvm.org (505) 553-7021
Director Sowers can confirm that DVM can discuss this option when the treatment is approved for medical cannabis therapy for seizures in animals. http://www.nmbvm.org/executive-director/
States Already Doing This: Colorado:
Colorado Veterinary Medical Association has been vocal about its stance on the issue as well. In an official 2016 position statement, the board declared that “veterinarians have an obligation to provide companion animal owners with complete education in regard to the potential risks and benefits of marijuana products in animals.” http://www.veterinarycannabis.org/uploads/4/3/5/9/43599201/cvma_position_statement_2017-01.pdf
California:
(Passed 2018 / Effect 2019) The bill requires the state veterinary board to develop guidelines by January 1, 2020 for practitioners to follow when discussing cannabis with clients. The law does not permit veterinarians to give cannabis or cannabis products to patients or their owners.
Conant v. Walters (2002): The Ninth Circuit Court of Appeals. “A physician may discuss the pros and cons of medical marijuana with his or her patient, and issue a written or oral recommendation to use marijuana within a bona fide doctor-patient relationship without fear of legal reprisal.” (https://www.safeaccessnow.org/landmark_federal_conant_v_walters)
Every year, the federal budget in the US Congress (“omnibus” appropriations bill) includes a rider that continues to bar the DOJ from enforcing the federal marijuana ban in some circumstances pertaining to states who enact their own medical cannabis laws. This rider is also known as the Rohrabacher–Farr amendment. Here is the full text of the rider: “SEC. 538. None of the funds made available under 4 this Act to the Department of Justice may be used, with respect to any of the States of Alabama, Alaska, Arizona, Arkansas, California, Colorado, Connecticut, Delaware, Florida, Georgia, Hawaii, Illinois, Indiana, Iowa, Kentucky, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nevada, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Oregon, Pennsylvania, Rhode Island, South Carolina, Tennessee, Texas, Utah, Vermont, Virginia, Washington, West Virginia, Wisconsin, and Wyoming, or with respect to the District of Columbia, Guam, or Puerto Rico, to prevent any of them from implementing their own laws that authorize the use, distribution, possession, or cultivation of medical marijuana.”
In United States v. McIntosh, the federal Ninth Circuit Court of Appeals interpreted the quoted language to bar the DOJ from prosecuting individuals who manufacture, distribute, or possess marijuana in strict compliance with state medical cannabis laws.
Petition Conclusion:
Approval of this Petition will Save Many Animal Lives in New Mexico...Tecumseh (my dog) has had 2 different DVM think he should have been put down last year, medical cannabis is saving his life.
Tecumseh’s (60 lbs) Current Medications (as of 09/11/19):
Phenobarbital 64.8 mg tablets; 162 mg given in 24 hr period. Tecumseh is given 1 1/2 tablet at 4 am and he is given 1 ¼ tablet at 4:00 pm.
Levetiracetam 750 mg Immediate Release; 3375 mg given in 24 hr period. Tecumseh is given 1500 mg (2 pills) 3 times a day at 4:30 am, 12:30 pm, and 8:30 pm.
Zonisamide 100 mg Capsule; Tecumseh is given 200 mg every 12 hrs. Tecumseh takes the Zonisamide twice a day at 6 am and 6 pm.
Clorazepate 7.5 mg (using/dosing at first sign of any seizure activity) Giving Tecumseh one, 7.5 mg, pill every 8 hours for 6 doses in 48 hrs.
IN Midazolam 1.5 mL of 5 mg/mL (using/dosing for seizure emergency)
Thats alot of pharmaceuticals… The approval of this Petition: Requesting The Inclusion Of A New Medical Treatment: Medical Cannabis Therapy For Seizures in Animals- that is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
And there is no aspect of the current medical cannabis program laws that would prevent this new medical treatment for Medical Cannabis Therapy For Seizures in Animals from being approved into the Medical Cannabis Program. Doctors of Veterinary Medicine are qualifying medical professionals who can recommend medical cannabis.- that is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
The approval of this petition will fulfill the intent of the law and uphold the integrity and spirit of the Lynn and Erin Compassionate Use Act, 2007.
Fulfilling both;“ Section 2. PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments”
And of section 6. ADVISORY BOARD CREATED--DUTIES: The advisory board shall: A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis.”
New Mexico’s medical cannabis history started in 1978. After public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis...the first law.
Jason Barker Albuquerque, NM SafeAccessNewMexico@gmail.com
Monday, November 11th 2019 (Petitions provided to NMDOH Medical Cannabis Program Office on November 12th 2019 via hand delivery)
New Mexico State Department of Health
Medical Cannabis Advisory Board Medical Cannabis Program PO Box 26110 Santa Fe, NM, 87502-6110
Petition: Requesting The Inclusion Of A New Medical Condition: Substance Abuse Disorder
(To Include: Alcohol Use Disorder (AUD), Tobacco Use Disorder, Stimulant Use Disorder, Hallucinogen Use Disorder, and Opioid Use Disorder)
Table of Contents
Pg. 1 Cover Page Pg. 2 Table of Contents Pg. 3 - 5 Petition Purpose and Background Pg. 5 - 7 Petition Background Information Pg. 6 - 7 Petition Background Information: Substance Abuse in New Mexico Pg. 8 UNM- Medical Cannabis Research Relevant to Petition Pg. 9 - 15 Introductory Narrative From Petitioner Pg. 15 - 19 About Substance Abuse Disorder Pg. 20 - 31 Supporting Articles Citing Research Pg. 31 - 41 Supporting Medical and Scientific Research Studies Pg. 41 - 51 Research For Cannabinoid Therapies & Substance Abuse Disorder Pg. 51 - 53 Conclusion: Cannabis Is A Exit Drug For Substance Abuse Pg. 53 - 54 Relief Requested In Petition Pg. 55 - 56 Appendix A: Alcohol Use in New Mexico Infographic Pg. 57 - 58 Appendix B: Prescription Monitoring Infographic Pg. 59 - 60 Appendix C: Drug Overdose in New Mexico Infographic Bonus Section: Healer Medical Cannabis Opioid Guide (8 Pages) Thousands of people have used cannabis to help them reduce and replace opioid medications, as demonstrated in numerous recent scientific papers and strongly supported by animal research (see guide for research). Dr. Sulak has created this guide to help you. Link: http://healer.com/wp-content/uploads/2018/04/Healer-Medical-Cannabis-Opioid-Guide.pdf
Petition Requesting The Inclusion Of A New Medical Condition: Substance Abuse Disorder
(To Include: Alcohol Use Disorder (AUD), Tobacco Use Disorder, Stimulant Use Disorder, Hallucinogen Use Disorder, and Opioid Use Disorder)
Mosby’s Medical Dictionary states that “medical treatment” means; the management and care of a patient to combat disease or disorder. Medical treatment includes: Using prescription medications, or use of a non-prescription drug at prescription strength; and or treatment of disease by hygienic and pharmacologic remedies, as distinguished from invasive surgical procedures. Treatment may be pharmacologic, using drugs; surgical, involving operative procedures; or supportive, building the patient's strength. It may be specific for the disorder, or symptomatic to relieve symptoms without effecting a cure.(Mosby's Medical Dictionary, 9th edition.)
What is a chronic medical condition? A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear. Harvard Medical Dictionary defines chronic as: Any condition that lasts a long time or recurs over time; chronic pain as: Pain that persists after an injury has healed or a disease is over; and chronic pain syndrome as : Long-term, severe pain that doesn't spring from an injury or illness, that interferes with daily life, and is often accompanied by other problems, such as depression, irritability, and anxiety.
What is the meaning of debilitating? Something that's debilitating seriously affects someone or something's strength or ability to carry on with regular activities, like a debilitating illness. Debilitating comes from the Latin word debilis, meaning "weak." That's why you'll often see the adjective used to describe illness, despite the negative reference.
The purpose of this Petition Requesting The Inclusion of a New Medical Condition: Substance Abuse Disorder; To Include: Alcohol Use Disorder (AUD), Tobacco Use Disorder, Stimulant Use Disorder, Hallucinogen Use Disorder, and Opioid Use Disorder (substance use disorder, for which the applicant or qualified patient is currently undergoing treatment for the applicant's or qualified patient's condition).
The purpose of this Petition Requesting The Inclusion of a New Medical Condition: Substance Abuse Disorder; To Include: Alcohol Use Disorder (AUD), Tobacco Use Disorder, Stimulant Use Disorder, Hallucinogen Use Disorder, and Opioid Use Disorder, is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
Who Should Qualify for Medical Cannabis Use? According to Americans For Safe Access Policy Studies & Research: (Americans For Safe Access is the largest national member-based organization of patients, medical professionals, scientists and concerned citizens promoting safe and legal access to cannabis for therapeutic use and research.)
Background: The most fundamental aspect of medical cannabis laws is the relationship between a patient and their physician. It is often only the physician and the patient that possess information about a patient’s health condition. However, many public officials and others who oppose medical cannabis laws often make assumptions about people’s health. The media have even fomented such inappropriate assumptions by naming a category of patients “Young Able Bodied Males,” condemning certain patients by visual assessment alone.
Findings: The health care information discussed between a patient and physician is considered private and protected under federal HIPAA laws. It is typically the purview of state medical boards to assess whether a physician has inappropriately recommended cannabis to someone who should not be qualified. Studies have shown in some medical cannabis states that the majority of patients suffer from chronic pain, an ailment that is not obviously detectable by another person. Nevertheless, police will often harass and arrest patients based on the assumption that someone is faking their illness.
Position: Medical professionals should have an unrestricted ability to recommend cannabis therapeutics and that should not be impacted by law enforcement’s perceptions.
Americans For Safe Access policy further states:
“Qualifying medical condition” shall mean any condition for which treatment with medical cannabis would be beneficial, as determined by a patient's qualified medical professional, including but not limited to cancer, glaucoma, positive status for human immunodeficiency virus, acquired immune deficiency syndrome (AIDS), hepatitis C, amyotrophic lateral sclerosis (ALS), Crohn’s disease, Parkinson’s disease, post-traumatic stress disorder, arthritis, chronic pain, neuropathic and other intractable chronic pain, and multiple sclerosis.
“Qualifying patient” shall mean a person who has a written recommendation from a qualified medical professional for the medical use of cannabis.
Petition Background Information: “Hemp Derived CBD vs. Cannabis Derived CBD - Where’s the Difference?”
Due to the heavy discussion in the Petition and research about CBD, here is a beneficial article summary about the scientific and medical differences of Hemp CBD and Cannabis CBD.
“Hemp Derived CBD vs. Cannabis Derived CBD - Where’s the Difference?”
“In terms of its molecular structure CBD is CBD is CBD—it’s the same molecule whether the CBD comes from hemp, cannabis or a test tube.”
“Whether the CBD comes from hemp or cannabis flowers is not the ultimate factor. The key factor is the process by which the CBD is extracted, concentrated and formulated. Cannabis strains such as Charlotte’s Web, Avidekel and ACDC are low in THC but high in CBD with up to a 20 percent CBD concentration level. By comparison, hemp’s typical 3.5 percent CBD concentration level is rather paltry.”
“Since the concentration of CBD is low in hemp, it requires large amounts of hemp to produce a small amount of CBD oil. The most efficient and least expensive way to extract the CBD oil is to use solvents, but dangerous solvent residues can remain in the CBD oil. In 2014, Project CBD, a California-based nonprofit dedicated to promoting and publicizing research into the medical uses of CBD, tested several CBD hemp oil products available to the public over the Internet and found significant levels of toxic solvent residues in random samples.”
“Even if it is possible to produce solvent-free CBD oil from hemp, there is another problem in that industrial hemp is a bio-accumulator that naturally absorbs toxic substances from the soil. Hemp is such an efficient bio-accumulator that it was used at the Chernobyl Nuclear power plant after the meltdown because it is excellent at sucking up heavy metals and radiation, according to McGraw Hill Education.”
“For many reasons, CBD-rich cannabis is a better source of CBD than industrial hemp. The only reason CBD derived from hemp is gaining any notoriety is as an attempted end-run around federal law. When cannabis prohibition is ended and cannabis is treated like any other agricultural product, CBD will be extracted from the best source of cannabidiol—CBD-rich cannabis. The need to derive CBD from industrial hemp will end.”
Petition Background Information: Substance Abuse in New Mexico Consequences of Substance Abuse Disorder Introduction All of the ten leading causes of death in New Mexico are, at least partially, attributable to the use of alcohol, tobacco, or other drugs. In 2016, the ten leading causes of death in New Mexico were diseases of the heart, malignant neoplasms, unintentional injuries, chronic lower respiratory diseases, cerebrovascular diseases, diabetes, Alzheimer’s disease, chronic liver disease and cirrhosis, suicide, and influenza and pneumonia. Of these, chronic liver disease, unintentional injuries, and suicide are associated with alcohol use; chronic lower respiratory diseases and influenza and pneumonia are associated with tobacco use; heart disease, malignant neoplasms, and cerebrovascular diseases are associated with both alcohol and tobacco use; and unintentional injuries and suicide are associated with the use of other drugs.
Alcohol-Related Deaths and Hospitalizations Over the past 30 years, New Mexico has consistently had among the highest alcohol-related death rates in the United States, and it has had the highest alcohol-related death rate since 1997. The negative consequences of excessive alcohol use in NM are not limited to death but also include domestic violence, crime, poverty, and unemployment, as well as chronic liver disease, motor vehicle crash and other injuries, mental illness, and a variety of other medical problems. In 2010, the economic cost of excessive alcohol consumption in New Mexico was $2.2 billion ($2.77 per drink or an average of $1,084 per person) (Sacks, Jeffrey J., et al. "2010 national and state costs of excessive alcohol consumption." American Journal of Preventive Medicine 49.5 (2015): e73-e79).
Smoking-Related Death Historically, New Mexico has had one of the lowest smoking-related death rates in the nation. Nonetheless, New Mexico’s burden of death associated with smoking is considerably greater than the burden associated with alcohol and other drugs. Among all racial/ethnic groups, males have higher smoking-related death rates than females. Among both males and females, Whites have the highest rates, followed by Blacks. The counties with the highest rates and relatively heavy burdens of smoking related death (i.e., 20 or more deaths a year) were Sierra, De Baca, Luna, Quay, Torrance, Eddy, and Lea. The high rates in most of these counties, and in the state overall, were driven by high rates among Whites.
Drug Overdose Death In 2017, New Mexico had the seventeenth highest drug overdose death rate in the nation. The consequences of drug use continue to burden New Mexico communities. Drug overdose death rates remained higher for males than for females. The highest drug overdose death rate was among Hispanic males. Rio Arriba County had the highest drug overdose death rate in the state. Bernalillo County continued to bear the highest burden of drug overdose death in terms of total numbers of deaths. Unintentional drug overdoses account for 88% of drug overdose deaths. The most common drugs causing unintentional overdose death for the period covered in this report were prescription opioids (i.e., methadone, oxycodone, morphine; 57%), heroin (40%), benzodiazepines (24%), cocaine (13%), and methamphetamine (26%) (not mutually exclusive). In New Mexico and nationally, overdose death from opioids has become an issue of enormous concern as these potent drugs are widely available.
Introductory Narrative From Petitioner Using the medical benefits of cannabis to treat Substance Abuse is not a new concept and is a concept that is over 20 years old in the making of this reality.
Suggested Reading That First Brought This Treatment Forward:
Dreher M. (2002). Crack heads and roots daughters: The therapeutic use of cannabis in Jamaica. Journal of Cannabis Therapeutics, 2(3/4):121-33.
Epstein DH & Preston KL. (2003). Does cannabis use predict poor outcomes for heroin-dependent patients on maintenance treatment? Past findings and more evidence against. Addiction, 98(3):269-79.
Labigalini E, Jr., Rodrigues LR & Da Silveira DX. (1999). Therapeutic use of cannabis by crack addicts in Brazil. Journal of Psychoactive Drugs, 31(4):451-5.
Mikuriya TH. (2004). Cannabis as a substitute for alcohol: a harm-reduction approach. Journal of Cannabis Therapeutics. 4(1):79-93.
Raby WN, Carpenter KM, Rothenberg J, Brooks AC, Jiang H, Sullivan M, Bisaga A, Comer S & Nunes EV. (2009). Intermittent marijuana use is associated with improved retention in naltrexone treatment for opiate-dependence. American Journal of Addictions, 18(4): 301-8
Medical Cannabis vs Prescriptions DrugsPrescription drug abuse is a serious and growing problem in the United States. The 2016 National Study on Drug Use and Health reported that an estimated 28.6 million Americans age 12 and over used illicit drugs during the month prior to the study. That means roughly 1 in 10 people struggle with some level of substance use, including addiction to prescription drugs.
When a person takes a prescription drug for a nonmedical reason, it can quickly lead to addiction and the need for drug treatment. In fact, 25 percent of people who misused prescription drugs by age 13 ended up with an addiction at some point in their life. (National Institute on Drug Abuse)
“More than 30 percent of overdoses involving opioids also involve benzodiazepines, a type of prescription sedative commonly prescribed for anxiety or to help with insomnia. Benzodiazepines (sometimes called "benzos") work to calm or sedate a person, by raising the level of the inhibitory neurotransmitter GABA in the brain. Common benzodiazepines include diazepam (Valium), alprazolam (Xanax), and clonazepam (Klonopin), among others.” March 2018 | NIDA | Link: https://www.drugabuse.gov/drugs-abuse/opioids/benzodiazepines-opioids
Article: ‘The Other Prescription Drug Problem: ‘Benzos’ Like Valium and Xanax’ “We’ve heard plenty about the opioid epidemic. But there’s another less recognized prescription drug problem: benzodiazepines like Ativan, Xanax, Valium, and Klonopin. While doctors are prescribing fewer painkillers, prescriptions for these anti-anxiety drugs are still going up. Besides anxiety, the Food and Drug Administration (FDA) has approved benzodiazepines for insomnia and other uses. They’re often prescribed alongside antidepressants. The quantity Americans consume has more than tripled since the mid-1990s. Benzos are involved in about a third of all deaths from prescription drug overdoses, typically combined with a painkiller. Both drugs may have been prescribed, since 17 percent of Americans with an opioid prescription also used a benzodiazepine in 2013. People also die when they take a benzo along with alcohol.”
Prescription Pills: Each year, about 4.5 million Americans visit their doctor’s office or the emergency room because of adverse prescription drug side effects. A startling 2 million other patients who are already hospitalized suffer the ill effects of prescription medications annually, and this when they should be under the watchful eye of medical professionals. The most common non-severe or mild side effects from taking drugs include (there are many more, these are the most common): Constipation, Dermatitis, Diarrhea, Dizziness, Drowsiness, Dry mouth, Headache, and Insomnia.
What are the short and long term effects of prescription drugs? Short-term effects: Alertness, focus, sleeplessness, loss of appetite, increased blood pressure and heart rate, high body temperature.
Long-term effects: Addiction, paranoia and long-term insomnia, extreme weight change.
What are the effects of prescription drugs? Physical symptoms: Increased or decreased need for sleep, Appearing unusually energetic, or overly fatigued, Increased or decreased appetite.
These drugs come with side effects that range from birth defects and liver damage to suicidal behavior, blood clots, bladder cancer, Crohn’s disease, heart attacks, strokes, uncontrollable bleeding, heart failure and death: Chronic Pain Treatment drug Fentanyl (opioid). Type 2 diabetes drugs Avandia and Actos. Antidepressants Paxil, Prozac, Effexor, Zoloft and Lexapro. Mood stabilizer Depakote. Birth control pills Yaz and Yasmin. Acne medication Accutane. Blood thinners Pradaxa and Xarelto Osteoporosis treatment Fosamax. GranuFlo and NaturaLyte, which are used in dialysis.
Hair loss pill Propecia. Stop smoking cigarettes drug Chantix.
In article in American-Statesman staff writer Jeremy Schwartz in 2012 noted that in 2011, “the Pentagon spent more on pills, injections and vaccines than it did on Black Hawk helicopters, Abrams tanks, Hercules C-130 cargo planes and Patriot missiles — combined.” The military spent at least $2.7 billion on antidepressants and more than $1.6 billion on opioid painkillers such as Oxycontin and hydrocodone over the past decade. More than $507 million was spent on the sleeping pill Ambien and its generic equivalents.” the pharmaceutical industry spent about $1.7 million for more than 1,400 trips for Defense Department doctors and pharmacists to places such as Paris, Las Vegas and New Orleans between 1998 and 2007. All those Pills have sadly killed a lot of our Veterans, Cannabis has a 5000 year history with zero deaths associated with it.
“Its margin of safety is immense and underscores the lack of any meaningful danger in using not only daily doses in the 3.5 – 9 gram range, but also considerably higher doses.”— David Bearman, M.D.(Physician, researcher, court-qualified cannabis expert) Link: http://www.davidbearmanmd.com/
Cannabis Is Safe & The Federal Government Has A Patent For It.
The U.S. Patent Office issuedpatent #6630507 to the U.S.Health and Human Services filed on 2/2/2001. The patent lists the use ofcannabinoids found within the plant cannabis sativa plant as useful in certain neurodegenerative diseases such as Alzheimer's, Parkinson's, and HIV dementia. Since cannabis sativa (marijuana) contains compounds recognized and endorsed by an agency of the U.S. government- Why is it that cannabis remains on the Federal Schedule One list of drugs? The issuance of patent #6630507 is a direct contradiction of the Government’s own definition for classification of a Schedule 1 drug. The U.S. government’s own National Institutes of Health researchers even concluded: “Based on evidence currently available the Schedule I classification is not tenable; it is not accurate that cannabis has no medical value, or that Information on safety is lacking.”
"The American Medical Association has no objection to any reasonable regulation of the medicinal use of cannabis and its preparations and derivatives. It does pretest, however, against being called upon to pay a special tax, to use special order forms in order to procure the drug, to keep special records concerning its professional use and to make special returns to the Treasury Department officials, as a condition precedent to the use of cannabis in the practice of medicine." (AMA Position Statement/Attempt To Prevent Prohibition) ~Wm. C. Woodward, Legislative Counsel - 11:37 AM Monday, July 12, 1937
Report: Medical Cannabis Research History. What the Science Says | Americans For Safe Access
It can be difficult to locate information about the safety and therapeutic value of cannabis. An unfortunate result of the federal prohibition of cannabis has been limited clinical research to investigate the safety and efficacy of cannabis to control symptoms of serious and chronic illness. Many scientists have noted research is “hindered by a complicated federal approval process, limited availability of research grade marijuana, and the debate over legalization.”
Nonetheless, the documented use of cannabis as a safe and effective therapeutic botanical dates to 2700 BC. Between 1840 and 1900, European and American journals of medicine published more than 100 articles on the therapeutic use of cannabis. In fact, cannabis was part of the American pharmacopoeia until 1942, and is currently available by prescription in Canada, the Netherlands, Israel, and Germany.
For over 5000 years, various strains of Cannabis have been among the most widely used of medicinal plants. This includes civilizations in China, India, Europe, Africa and the Middle East. Cannabis was used in the US from 1800’s to 1937 to treat more than 100 distinct diseases or conditions.
Cannabis is a NON-TOXIC substance. No one has ever died from taking cannabis. One hundred per cent of the scores of studies by American universities and research facilities show that toxicity does not exist in cannabis. (U.C.L.A, Harvard, Temple, etc.) All the in-depth medico-scientific clinical studies conducted (for example, US-Jamaican, US-Costa Rican, LaGuardia Report, etc) have revealed that cannabis contains no addictive properties in any part of the plant or its smoke, so, unlike and in contrast to tobacco, alcohol, and all the legal or illegal 'recreational' substances cannabis is both non-habit-forming and non-toxic.
Therefore cannabis is uniquely safe when compared to modern FDA approved prescriptions.
Cannabis stimulate CB1 and CB2 endocannabinoid receptors on the brain and other tissues that affect body systems, triggering a chain of temporary psychological and physiological effects. Initially it has a stimulant effect, followed by relaxation and overall reduction in stress. Analgesic effect. Blocks migraine or seizures. Helps mitigate or control symptoms of multiple sclerosis (MS), spinal injury, epilepsy. Lifts mood and enhances sense of well-being. Relieves chronic and neuropathic pain. Has synergistic effects with opiates and other drugs. Not all cannabis has the same potency or effect. May cause drowsiness, distraction, paranoia or anxiety (due to type of cannabis strain) and dry mouth - that’s it.
Americans for Safe Access (ASA) released the Medical Cannabis Access for Pain Treatment: A Viable Strategy to Address the Opioid Crisis report to educate legislators and health practitioners on the benefits of medical cannabis as a treatment option for the millions of patients suffering from chronic pain. Prescription opioid use has increased dramatically over the last two decades, and in the same period the number of deaths attributed to opioid overdose have quadrupled, creating a national crisis.
In a briefing released earlier this year, President Obama proposed $1.1B in new funding for a multi-pronged approach to address the opioid overdose epidemic. In July, Obama signed the Comprehensive Addiction and Recovery Act (CARA) into law. Many of the provisions in CARA focus on post-addiction strategies for treating drug abuse, heroin use, and overdose prevention strategies. Provisions that focus upstream, including addiction prevention strategies and ways to reduce the amount of opioids prescribed while still ensuring patients receive effective treatment, are underrepresented in the plan. While increasing funding for treatment programs is critical, it is equally important to utilize less harmful, treatment options.
ASA’s report outlines research and data supporting cannabis as an effective treatment option and provides three recommendations:
Pass the Compassionate Access, Research Expansion, and Respect States (CARERS) Act (S.683), Include Chronic Pain as a Qualifying Condition in State Medical Cannabis Laws Promote Medical Cannabis Education through State Medical Boards
“We know that patients across the US are successfully utilizing cannabis to treat pain” said ASA’s Executive Director Steph Sherer. “ It is not a coincidence that opiate deaths are down nearly 25% in the states that allow medical professionals and their patients to utilize cannabis therapies as a treatment option. The Medical Cannabis Access for Pain Treatment: A Viable Strategy to Address the Opioid Crisis report shows that access to medical cannabis for pain treatment would help address two major components of the opiate crisis; accidental overdoses and addiction.”
About Substance Use Disorder:(To Include: Alcohol Use Disorder (AUD), Tobacco Use Disorder, Stimulant Use Disorder, Hallucinogen Use Disorder, and Opioid Use Disorder.)
Substance Use Disorder is a complex brain disease and includes such diseases as alcoholism and drug addiction. Substance Use Disorders occur when a person has a dependence on alcohol and or drugs that is accompanied by intense and sometimes uncontrollable cravings and compulsive behaviors to obtain the substance.
These behaviors fall into four main categories: 1. Impaired control 2. Social impairment 3. Risky use 4. Pharmacological indicators (tolerance and withdrawal) Criteria for Substance Use Disorders
Substance use disorders span a wide variety of problems arising from substance use, and cover 11 different criteria:
Taking the substance in larger amounts or for longer than you're meant to
Wanting to cut down or stop using the substance but not managing to
Spending a lot of time getting, using, or recovering from use of the substance
Cravings and urges to use the substance
Not managing to do what you should at work, home, or school because of substance use
Continuing to use, even when it causes problems in relationships
Giving up important social, occupational, or recreational activities because of substance use
Using substances again and again, even when it puts you in danger
Continuing to use, even when you know you have a physical or psychological problem that could have been caused or made worse by the substance
Needing more of the substance to get the effect you want (tolerance)
Development of withdrawal symptoms, which can be relieved by taking more of the substance
Background and Types of Substance Use Disorders The following is a list with descriptions of the most common substance use disorders in the United States. Alcohol Use Disorder (AUD)
Excessive alcohol use can increase a person’s risk of developing serious health problems in addition to those issues associated with intoxication behaviors and alcohol withdrawal symptoms. According to the Centers for Disease Control and Prevention (CDC), excessive alcohol use causes 88,000 deaths a year.
Data from the National Survey on Drug Use and Health (NSDUH) — 2014 (PDF | 3.4 MB) show that in 2014, slightly more than half (52.7%) of Americans ages 12 and up reported being current drinkers of alcohol. Most people drink alcohol in moderation. However, of those 176.6 million alcohol users, an estimated 17 million have an AUD.
Many Americans begin drinking at an early age. In 2012, about 24% of eighth graders and 64% of twelfth graders used alcohol in the past year.
The definitions for the different levels of drinking include the following:
Moderate Drinking—According to the Dietary Guidelines for Americans, moderate drinking is up to 1 drink per day for women and up to 2 drinks per day for men.
Binge Drinking—SAMHSA defines binge drinking as drinking 5 or more alcoholic drinks on the same occasion on at least 1 day in the past 30 days. The National Institute on Alcohol Abuse and Alcoholism (NIAAA) defines binge drinking as a pattern of drinking that produces blood alcohol concentrations (BAC) of greater than 0.08 g/dL. This usually occurs after 4 drinks for women and 5 drinks for men over a 2 hour period.
Heavy Drinking—SAMHSA defines heavy drinking as drinking 5 or more drinks on the same occasion on each of 5 or more days in the past 30 days.
Excessive drinking can put you at risk of developing an alcohol use disorder in addition to other health and safety problems. Genetics have also been shown to be a risk factor for the development of an AUD.
To be diagnosed with an AUD, individuals must meet certain diagnostic criteria. Some of these criteria include problems controlling intake of alcohol, continued use of alcohol despite problems resulting from drinking, development of a tolerance, drinking that leads to risky situations, or the development of withdrawal symptoms. The severity of an AUD—mild, moderate, or severe—is based on the number of criteria met. Tobacco Use Disorder
According to the CDC, more than 480,000 deaths each year are caused by cigarette smoking. Tobacco use and smoking do damage to nearly every organ in the human body, often leading to lung cancer, respiratory disorders, heart disease, stroke, and other illnesses.
In 2014, an estimated 66.9 million Americans aged 12 or older were current users of a tobacco product (25.2%). Young adults aged 18 to 25 had the highest rate of current use of a tobacco product (35%), followed by adults aged 26 or older (25.8%), and by youths aged 12 to 17 (7%).
In 2014, the prevalence of current use of a tobacco product was 37.8% for American Indians or Alaska Natives, 27.6% for whites, 26.6% for blacks, 30.6% for Native Hawaiians or other Pacific Islanders, 18.8% for Hispanics, and 10.2% for Asians. Stimulant Use Disorder
Stimulants increase alertness, attention, and energy, as well as elevate blood pressure, heart rate, and respiration. They include a wide range of drugs that have historically been used to treat conditions, such as obesity, attention deficit hyperactivity disorder and, occasionally, depression. Like other prescription medications, stimulants can be diverted for illegal use. The most commonly abused stimulants are amphetamines, methamphetamine, and cocaine. Stimulants can be synthetic (such as amphetamines) or can be plant-derived (such as cocaine). They are usually taken orally, snorted, or intravenously.
In 2014, an estimated 913,000 people ages 12 and older had a stimulant use disorder because of cocaine use, and an estimated 476,000 people had a stimulant use disorder as a result of using other stimulants besides methamphetamines. In 2014, almost 569,000 people in the United States ages 12 and up reported using methamphetamines in the past month.
Symptoms of stimulant use disorders include craving for stimulants, failure to control use when attempted, continued use despite interference with major obligations or social functioning, use of larger amounts over time, development of tolerance, spending a great deal of time to obtain and use stimulants, and withdrawal symptoms that occur after stopping or reducing use, including fatigue, vivid and unpleasant dreams, sleep problems, increased appetite, or irregular problems in controlling movement. Hallucinogen Use Disorder
Hallucinogens can be chemically synthesized (as with lysergic acid diethylamide or LSD) or may occur naturally (as with psilocybin mushrooms, peyote). These drugs can produce visual and auditory hallucinations, feelings of detachment from one’s environment and oneself, and distortions in time and perception.
In 2014, approximately 246,000 Americans had a hallucinogen use disorder. Symptoms of hallucinogen use disorder include craving for hallucinogens, failure to control use when attempted, continued use despite interference with major obligations or social functioning, use of larger amounts over time, use in risky situations like driving, development of tolerance, and spending a great deal of time to obtain and use hallucinogens. Opioid Use Disorder
Opioids reduce the perception of pain but can also produce drowsiness, mental confusion, euphoria, nausea, constipation, and, depending upon the amount of drug taken, can depress respiration. Illegal opioid drugs, such as heroin and legally available pain relievers such as oxycodone and hydrocodone can cause serious health effects in those who misuse them. Some people experience a euphoric response to opioid medications, and it is common that people misusing opioids try to intensify their experience by snorting or injecting them. These methods increase their risk for serious medical complications, including overdose. Other users have switched from prescription opiates to heroin as a result of availability and lower price. Because of variable purity and other chemicals and drugs mixed with heroin on the black market, this also increases risk of overdose. Overdoses with opioid pharmaceuticals led to almost 17,000 deaths in 2011. Since 1999, opiate overdose deaths have increased 265% among men and 400% among women.
In 2014, an estimated 1.9 million people had an opioid use disorder related to prescription pain relievers and an estimated 586,000 had an opioid use disorder related to heroin use.
Symptoms of opioid use disorders include strong desire for opioids, inability to control or reduce use, continued use despite interference with major obligations or social functioning, use of larger amounts over time, development of tolerance, spending a great deal of time to obtain and use opioids, and withdrawal symptoms that occur after stopping or reducing use, such as negative mood, nausea or vomiting, muscle aches, diarrhea, fever, and insomnia.
Article 1: ‘New potential for marijuana: Treating drug addiction’ By Susan Scutti, CNN | Updated 7:21 PM ET, Wed May 17, 2017
(CNN) Harm reduction is a strategy for treating addiction that begins with acceptance. A friendlier, less disciplined sister of abstinence, this philosophy aims to reduce the overall level of drug use among people who are unable or simply unwilling to stop. What should naturally follow is a decrease in the many negative consequences of drug use.
Most European countries and Canada have embraced the idea of harm reduction, designing policies that help people with drug problems to live better, healthier lives rather than to punish them.
On the front lines of addiction in the United States, some addiction specialists have also begun to work toward this end.
Joe Schrank, program director and founder of High Sobriety, is one of them. He says his Los Angeles-based treatment center uses medicinal cannabis as a detox and maintenance protocol for people who have more severe addictions, although it's effectiveness is not scientifically proven.
"So it's a harm-reduction theory," he said. "With cannabis, there is no known lethal dose; it can be helpful for certain conditions."
Still, harm reduction is gaining acceptance in the wider field of addiction specialists in the U.S.
"In principle, what we have aimed for many years is to find interventions that would lead to complete abstinence," said Dr. Nora Volkow, director of the National Institute on Drug Abuse. Practically, though, that has been very difficult to achieve with relapsing addictions.
"One of the things is, we don't have any evidence-based medication that has proven to be efficacious for the treatment of cocaine addiction," Volkow said. "So we currently have no medicine to intervene, and it can be a very severe addiction and actually quite dangerous."
Dangerous because it gives users a high that literally alters the brain. Medical consequences of cocaine addiction include seizure, stroke and bleeding within the brain.
"We have started to explore the extent to which interventions that can decrease the amount of drug consumed can have benefits to the individual," Volkow said, adding that she'd make this same argument for opioids and heroin. "It would be valuable to decrease the amount of drug consumed."
Schrank is clear on the value of simply reducing drug use.
"We think of addiction as this light switch you can turn on and off," he said. "What we're learning is that for some people, it's similar to scuba diving: You can only come up 20 feet so often or you get very, very sick. When people stop immediately and that abruptly, it really makes them vulnerable."
Schrank, who readily concedes there are possible health and addiction risks with marijuana, says he offers his cannabis detox and maintenance protocol to people addicted to crack cocaine as well as those trying to kick opioids. Through the years, he says, he's treated about 50 people with this technique and expects to see "more people wanting to try to have a voice in their recovery rather than just plug into systems telling them what to do."
Marijuana "can really help people with pain management and other health issues, or it can help them be safer," Schrank said. Reversing heroin's damage
Yasmin Hurd, director of the Addiction Institute at Mount Sinai School of Medicine, says generally, cannabidiol is the more important compound when it comes to marijuana as a treatment for addiction. It is one of the two primary cannabinoids, along with Δ9-tetrahydrocannabinol (THC), found in the cannabis plant. In terms of the wider scope of medical marijuana research, this is the "same cannabidiol being looked at for the kids with epilepsy," Hurd said.
THC, she says, binds to cannabinoid receptors in our brains (as do the natural cannabinoids our bodies produce), and it is the stimulation of those receptors that brings a "high." By comparison, cannabidiol has very weak effects in this regard and negatively modulates that receptor, instead.
For instance, heroin harms the glutamate transmitter system, which is important for decision-making, cognition and even reward, explains Hurd.
"We found that (cannabidiol) reversed the impairments caused by heroin, for example, on the glutamatergic receptors," Hurd said. Similarly, cannabidiol reversed damage to the cannabinoid receptors themselves caused by heroin, while activating the serotonin system: the neurotransmitter system believed to affect mood and a common target for makers of anti-anxiety and antidepressant medications.
More generally, cannabidiol positively influences our biological systems that are linked to the negative components of addiction, such as anxiety and inhibitory control, Hurd suggests.
"We still haven't figured out how it works," Hurd said. She notes that although cannabidiol is believed to be a "treatment to consider for opioid addiction and other drugs," there aren't a lot of data, especially with regard to its potential effects for cocaine addiction.
Adding to the data is a recent study, funded in part by a company applying to the Canadian government for a license to produce medical cannabis, exploring one possible harm reduction plan: swapping crack cocaine for marijuana.
Article 2: ‘High Sobriety: A Path Toward Life and Choice.’
(From the California Program Currently Treating Addiction with Medical Cannabis)
“High Sobriety supports a spectrum of recovery alternatives for individuals who have been previously unable to stop using alcohol and/or other drugs after attending traditional abstinence-based settings. The sheer number of people that fall into this category is astounding. For example, if you examine statistics from SAMHSA (Substance Abuse & Mental Health Services Administration), approximately 25% of individuals who undergo abstinence-based treatment, do not relapse. Although any measure of success is encouraging, we at High Sobriety are committed to supporting the remaining 75%, who incidentally, rank in the millions.
Tradition Vs. Change
The majority of other recovery programs are staffed with “recovering” addicts and alcoholics. Most of these individuals participate (hopefully) in a 12-Step Program, which they believe, is the one path that helped them get clean and sober. Therefore, when a client questions the concept of total abstinence, the staff member will shut it down, citing no real data, except for their own personal experience in 12-Step Meetings.
Herein lies the crux of the problem; individuals that don’t adhere to the concept of total abstinence, but have improved their lives, do not attend 12-Step Meetings. They are not welcome there, unless of course, they want to stop doing what has worked for them, and adhere to a confusing set of internally known but publicly unsung standards about which types of drugs are acceptable in the 12-Step Program and when they can be used. For example, a benzodiazepine prescribed by a Psychiatrist for the treatment of anxiety is probably reasonable, but cannabis prescribed for Crohn’s Disease or a Sleep Disorder is definitely not!
Although these standards may make sense to most traditional practitioners working in traditional treatment settings, they don’t make a lot of sense when considering the needs of the 75% who don’t understand the concept of abstinence, and more importantly, have probably demonstrated an inherent inability to abide by that philosophy in the past.
We support our residents’ cannabis replacement approach, where it is in full compliance with law and under medical supervision. Cannabis is used for a variety of medical conditions for treating and aiding symptomatic care. Cannabis can aid in the cleansing process, helping with discomfort, insomnia, and flu-like symptoms associated with the withdrawal process, reducing or eliminating the need for other drugs. After the initial cleansing process, a doctor of the residents’ choice provides a comprehensive and collaborative evaluation to determine an individual’s goals for recovery. The determination of how cannabis is used is ultimately made by the doctor, like any other medication.
Post cleansing, cannabis continues to be an option under medical supervision. When someone has been using for a prolonged period of time, moving into total abstinence within 30 days may not be a realistic undertaking, it may not even be the best strategy. It certainly raises the question: if total abstinence is the best course of action, why are the results so poor?”
Article 3: ‘How Cannabis Can Combat the Opioid Epidemic: An Interview With Philippe Lucas’ | Leafly
Philippe Lucas has deep roots in Canada’s cannabis culture. After co-founding the Vancouver Island Compassion Society medical dispensary in 1999, Lucas applied himself to cannabis science, working as a graduate researcher with the Center for Addictions Research of British Columbia and serving as founding board member of both the Multidisciplinary Association of Psychedelic Studies Canada and the Canadian Drug Policy Coalition. In 2013, he received the Queen Elizabeth II Diamond Jubilee Medal for his research on medical cannabis.
(Full disclosure/fun fact: He’s also Vice President of Patient Advocacy at Tilray, the cannabis production company owned by Privateer Holdings, which also owns Leafly.)
Most recently, Lucas is the author of a new study: “Rationale for cannabis-based interventions in the opioid overdose crisis,” published last month in the Harm Reduction Journal. In the study, Lucas lays out a variety of roles that cannabis might play in combating the opioid epidemic, which currently kills 38,000 people in the U.S. and Canada each year and ranks as the leading cause of death among Americans under 50.
His study added an important perspective to the growing body of evidence supporting the notion of cannabis as healing tool in the opioid crisis. That idea is quickly moving into mainstream thought, as we’ve seen recently with the public pronouncements of Utah Sen. Orrin Hatch and, just this week, Dr. Oz.
Over the phone from his office in Nanaimo, Lucas let me interrogate him about specifics of the study.
Dave Schmader: What inspired you to undertake this study?
Philippe Lucas: Whether it’s medical use or recreational use, cannabis appears to be having an impact on the rates of opioid abuse. This study is a summation of the evidence, and I’ve taken that summation to suggest three opportunities for cannabis to intervene in the opioid crisis.
And those are…?
First is introduction—if physicians start recommending the use of medical cannabis prior to introducing patients to opioids, those patients that find cannabis to be a successful treatment for their chronic pain might never have to walk down the very tricky path of opioid use that all too often leads to abuse or using to much or overdose.
“Patients that find cannabis to be a successful treatment for their chronic pain might never have to walk down the very tricky path of opioid use.”
The second opportunity is reduction, for those patients who are successfully using opioids in the treatment of their chronic pain or other conditions but are worried about increasing their use of opioids over time. The evidence suggests you can introduce cannabis as an adjunct treatment and reduce the cravings for opioids, therefore potentially steering people away and reducing the risk of opioid overdose and opioid dependence.
The third part is cessation. Once individuals have become dependent on opioids and they recognize that dependence and are seeking treatment for it through opioid replacement therapy like methadone and suboxone, you can potentially introduce cannabis as an adjunct treatment to increase the success rate of the methadone or suboxone treatment. The reason this point is so important is that when people with an opioid dependence fail out of treatment, that’s the period where they become the most vulnerable to potential overdose. Replacement therapy has failed, they’re at their most vulnerable, and they go back to the illicit drug market, potentially risking overdose.
A key concept in the study is the “substitution effect.”
Yes. The substitution effect is an economic concept that suggests that the use of one substance never stands alone. In fact, the use of one substance can affect the use of another. When it comes to psychoactive substances, the use of a substance can be affected by changes in price, changes in legality or regulatory access, or changes in the product itself in terms of potency. And that can really affect the use of another drug.
“In medical cannabis states, there was a 25 percent reduction in opioid overdose deaths.”
A 2014 study showed that in medical cannabis states, there was a 25 percent reduction in opioid overdose deaths compared to neighboring states that didn’t have medical cannabis programs. There’s a growing body of research showing that simply making medical cannabis available in a number of US states and in Canada has reduced rates of not just opioid use, but also the use of alcohol, tobacco, and illicit substances,
often leading to total abstinence of those substances. So we’re looking at cannabis as a potential therapeutic agent, but also as a harm reduction agent when it comes to problematic substance use. This evidence suggests cannabis could be an exit drug to problematic substance use and addiction.
In the study you write, “Cannabis augments the pain-relieving potential of opioids and can re-potentiate their effects.” Tell me about re-potentiation.
Research suggests that when you use cannabis alongside opioids in the treatment of chronic pain, you seem to get a synergistic effect—a greater effect than you might have if each was taken individually. People who have been using opioids for some time sometimes have to increase their dose, and cannabis presents another option for physicians, so instead of increasing the dose of opioids they can instead prescribe medical cannabis as an adjunct treatment in order to keep the patient at a lower dose of opioids, thereby reducing the risk of overdose.
Another study quote: “It would seem logical to seek to develop policies and associated education strategies to increase physician support for cannabis for therapeutic purposes in the treatment of chronic pain.” This does seem logical. What are the chances of it happening?
Right now we’re facing this tremendous public-health threat around the opioid overdose crisis. Opioid overdose is the most common cause of accidental death in Canada and the US right now. The over-prescription of opioids seems to be leading the way, in that four out of five people currently injecting opioids say that they started by using prescription opioids. There’s an oversaturation of the market and an over-availability on the black market.
I think that if we can shift prescription patterns by physicians—so that instead of first prescribing opioids and then, if those opioids fail, moving on to medical cannabis—we can modernize those policies and instead focus on introducing medical cannabis first. That’s based on all the available evidence, which indicates that it’s far less harmful than prescription opioids in terms of dependence and risk of overdose.
Right now in Canada and in US states with medical marijuana, physicians are encouraged to prescribe opioids first and if those don’t work, cannabis is considered as a third- or fourth-line treatment option. We need to flip that around and make cannabis the second-line treatment option and move opioids to third or fourth options if indeed cannabinoids are not successful.
Figure 1: When THC and prescription opioids are co-administered, the same level of pain relief is achieved with lower opioid dosage. This can prevent some of the negative side effects of opioid treatment and allow patients to reduce opioid use. (Photo credit: Amy Phung/Leafly)
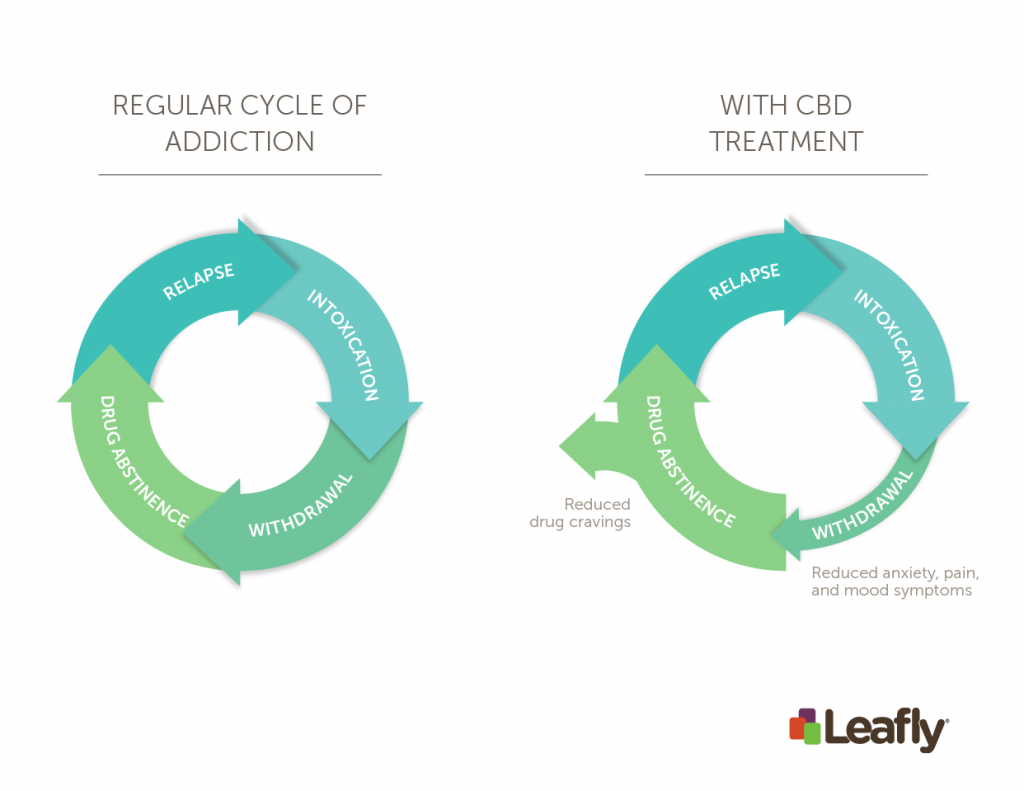
Figure 2: CBD treatment can reduce the chance of relapse for those struggling with drug addiction by altering the withdrawal and drug abstinence phases. Symptoms of withdrawal will be treated, decreasing pain, anxiety, and mood symptoms. CBD can promote drug abstinence by reducing drug craving through suppression of the reward system of the brain. (Photo credit: Amy Phung/Leafly) Source: https://www.leafly.com/news/health/how-cannabis-can-combat-the-opioid-epidemic-an-interview-with-philippe-lucas
Article/Video 4: “How Medical Cannabis Can Cure the Opioid Epidemic with Dr. Jacob Vigil”
Drs. Jacob Vigil, Anthony Reeve, and Sarah Stith talk about how medical cannabis can treat chronic pain and stop the opioid epidemic (Youtube Video). Visit the University of New Mexico Medical Cannabis Research Fund at: mcrf.unm.edu
Article 5: “Study Finds Medical Cannabis May Reduce Use Of Dangerous Prescription Drugs”
The United States is in the midst of a major drug epidemic. Stories continue to roll in daily about the lives claimed by prescription and non-prescription drug overdoses. The numbers are staggering. Opioids alone (including prescription painkillers and street heroin) killed more than 33,000 people in 2015, 90+ Americans every single day, and more than any year on record according to the Center for Disease Control (CDC). From 2000 to 2015, half a million people died from prescription drug overdoses.
The opioid epidemic is the leading preventable form of death in the United States.
“The potential for addiction and health risks associated with using multiple scheduled drugs places additional direct monetary and health costs on patients and healthcare systems due to an increased number of side effects, risky drug interactions, dependency, and overdose” stated University of New Mexico researchers Jacob Miguel Vigil and Sarah See Stith, of a new study titled, Effects of Legal Access to Cannabis on Scheduled II-V Drug Prescriptions, which will be soon released in an upcoming issue of the Journal of American Medical Directors Association.
The study resulted from insights provided by co-investigator Dr. Anthony Reeve, a pain specialist from the Industrial Rehabilitation Pain Clinics, Albuquerque, N.M. and also one of the first physicians to authorize the use of cannabis for patients with chronic pain in the state of New Mexico.
Reeve observed a number of his patients coming back to see him, not only less frequently after enrolling in the New Mexico Medical Cannabis Program (MCP), but anecdotally, they would often claim that they were not only reducing their pain medications, but other types of prescription medications as well.
In their historical cohort study the researchers compared individuals that enrolled in the medical cannabis program to individuals with a similar diagnosis that chose not to enroll in the medical cannabis program but were offered the same authorization, to measure the effect of enrollment in a state-authorized United States’ MCP on Scheduled II-V drug prescription patterns.
They compared 83 chronic pain patients, who enrolled in the New Mexico Medical Cannabis Program during a five+ year period from April 2010 to October 2015, to 42 non-enrolled patients over a 24 month period (starting 6 months prior to enrollment for the MCP patients) using the Prescription Monitoring Program.
Using outcome variables including baseline levels and pre- and post-enrollment monthly trends in the numbers of drug prescriptions, distinct drug classes, dates prescription drugs were filled, and prescribing providers, the researchers found that 28 cannabis program enrollees (34 percent) and one comparison group patient (2 percent) ceased the use of all scheduled prescription medications by the last six months of the observation period.
Age and gender-adjusted regressions show that, although no statistically significant differences existed in pre-enrollment levels and trends, the post-enrollment trend among MCP patients is statistically significantly negative for all four measures of scheduled drug medication usage, while the post-enrollment trend is zero among the comparison group. The cannabis program enrollees showed statistically significantly lower levels across all four measures in comparison to the non-enrollees by 10 months post-enrollment. The researchers hypothesize that legal access to cannabis may reduce the use of multiple classes of dangerous prescription medications in certain patient populations.
“Our current opioid epidemic is the leading preventable form of death in the United States, killing more people than car accidents and gun violence,” said Vigil, the senior author and Associate Professor in the Department of Psychology. “No one has ever died from smoking too much cannabis. Therefore, the relative safety and efficacy of using cannabis in comparison to that of the other scheduled medications should be taken by the health providers and legislators, and may very well to have been considered by the patients in our study.”
The authors state that increased patient access to MCPs could impact prescription drug activity in numerous ways. “Potentially, MCPs might drive increased prescribing of medications as a result of side effects of cannabis use, including agitation or somnolence. Alternatively, access to cannabis could lead to a reduction in scheduled prescription drug use, if it treats patients’ underlying condition(s) more effectively than scheduled drugs requiring a prescription.”
The researchers are currently employing naturalistic studies to identify how older patients use and are affected by opioids, benzodiazepines, and medical cannabis for treating significant and societally expensive health conditions.
Americans for Safe Access and the U.S. Pain Foundation launched the End Pain Not Lives campaign on November 1, 2017, to address the root of the opioid epidemic in the United States.
The epidemic is claiming over 130 lives a day.
Current public health policies focus solely on downstream strategies and criminalizing patients and medical professionals. Yet the research shows a nearly 25% decrease of opioid overdose deaths in states with medical cannabis laws. However, medical cannabis is not option for all patients due to the federal-state legal conflict, inadequacies in state laws, and lack of medical professional and patient education.
Supporting Medical and Scientific Research Studies1. ‘Cannabidiol as a Novel Candidate Alcohol Use Disorder Pharmacotherapy: A Systematic Review’ Published: 30 January 2019 | https://doi.org/10.1111/acer.13964
Abstract There is substantial interest in the therapeutic potential of cannabidiol (CBD), a nonpsychoactive cannabinoid found in plants of the genus Cannabis. The goal of the current systematic review was to characterize the existing literature on this topic and to evaluate the credibility of CBD as a candidate pharmacotherapy for alcohol use disorder (AUD). Using a comprehensive search strategy, 303 unique potential articles were identified and 12 ultimately met criteria for inclusion (8 using rodent models, 3 using healthy adult volunteers, and 1 using cell culture). In both rodent and cell culture models, CBD was found to exert a neuroprotective effect against adverse alcohol consequences on the hippocampus. In rodent models, CBD was found to attenuate alcohol‐induced hepatotoxicity, specifically, alcohol‐induced steatosis. Finally, findings from preclinical rodent models also indicate that CBD attenuates cue‐elicited and stress‐elicited alcohol seeking, alcohol self‐administration, withdrawal‐induced convulsions, and impulsive discounting of delayed rewards. In human studies, CBD was well tolerated and did not interact with the subjective effects of alcohol. Collectively, given its favorable effects on alcohol‐related harms and addiction phenotypes in preclinical models, CBD appears to have promise as a candidate AUD pharmacotherapy. This is further bolstered by the absence of abuse liability and its general tolerability. A clear limitation to the literature is the paucity of human investigations. Human preclinical and clinical studies are needed to determine whether these positive effects in model systems substantively translate into clinically relevant outcomes.
2. ‘Pills to Pot: Observational Analyses of Cannabis Substitution Among Medical Cannabis Users With Chronic Pain’ |Published 011019 | DOI: https://doi.org/10.1016/j.jpain.2019.01.010
Highlights •Medical cannabis users reported substituting cannabis for pain medications. •User rationale for substitution was fewer side effects and better pain management. •Most users reported improved pain and health since using cannabis. •Intentions behind and duration of cannabis use affected substitution behavior. •Unlike previous studies, >50% of participants were women and adults >50 years old. Abstract Chronic pain is common, costly, and challenging to treat. Many individuals with chronic pain have turned to cannabis as an alternative form of pain management. We report results from an ongoing, online survey of medical cannabis users with chronic pain nationwide about how cannabis affects pain management, health, and pain medication use. We also examined whether and how these parameters were affected by concomitant recreational use, and duration of use (novice: <1 year vs experienced: ≥1 year). There were 1,321 participants (59% female, 54% ≥50 years old) who completed the survey. Consistent with other observational studies, approximately 80% reported substituting cannabis for traditional pain medications (53% for opioids, 22% for benzodiazepines), citing fewer side effects and better symptom management as their rationale for doing so. Medical-only users were older (52 vs 47 years old; P < .0001), less likely to drink alcohol (66% vs 79%, P < .0001), and more likely to be currently taking opioids (21% vs 11%, P < .0001) than users with a combined recreational and medical history. Compared with novice users, experienced users were more likely to be male (64% vs 58%; P < .0001), take no concomitant pain medications (43% vs 30%), and report improved health (74% vs 67%; P = .004) with use. Given that chronic pain is the most common reason for obtaining a medical cannabis license, these results highlight clinically important differences among the changing population of medical cannabis users. More research is needed to better understand effective pain management regimens for medical cannabis users.
Perspective: This article presents results that confirm previous clinical studies suggesting that cannabis may be an effective analgesic and potential opioid substitute. Participants reported improved pain, health, and fewer side effects as rationale for substituting. This article highlights how use duration and intentions for use affect reported treatment and substitution effects.
3. ‘Medical cannabis patterns of use and substitution for opioids & other pharmaceutical drugs, alcohol, tobacco, and illicit substances; results from a cross-sectional survey of authorized patients’ | Harm Reduction Journal 2019 | https://doi.org/10.1186/s12954-019-0278-6
Abstract
Background: A 239-question cross-sectional survey was sent out via email in January 2017 to gather comprehensive information on cannabis use from Canadian medical cannabis patients registered with a federally authorized licensed cannabis producer, resulting in 2032 complete surveys. Methods: The survey gathered detailed demographic data and comprehensive information on patient patterns of medical cannabis use, including questions assessing the self-reported impact of cannabis on the use of prescription drugs, illicit substances, alcohol, and tobacco. Results: Participants were 62.6% male (n = 1271) and 91% Caucasian (n = 1839). The mean age was 40 years old, and pain and mental health conditions accounted for 83.7% of all respondents (n = 1700). Then, 74.6% of respondents reported daily cannabis use (n = 1515) and mean amount used per day was 1.5 g. The most commonly cited substitution was for prescription drugs (69.1%, n = 953), followed by alcohol (44.5%, n = 515), tobacco (31.1%, n = 406), and illicit substances (26.6%, n = 136). Opioid medications accounted for 35.3% of all prescription drug substitution (n = 610), followed by antidepressants (21.5%, n = 371). Of the 610 mentions of specific opioid medications, patients report total cessation of use of 59.3% (n = 362). Conclusions :This study offers a unique perspective by focusing on the use of a standardized, government-regulated source of medical cannabis by patients registered in Canada’s federal medical cannabis program. The findings provide a granular view of patient patterns of medical cannabis use, and the subsequent self-reported impacts on the use of opioids, alcohol, and other substances, adding to a growing body of academic research suggesting that increased regulated access to medical and recreational cannabis can result in a reduction in the use of and subsequent harms associated with opioids, alcohol, tobacco, and other substances.
4. ‘Opioid dose reduction and pain control with medical cannabis.’ | Journal of Clinical Oncology | November 28, 2018 |DOI: 10.1200/JCO.2018.36.34_suppl.189 Journal of Clinical Oncology 36, no. 34_suppl (December 1 2018) 189-189.
Abstract:
Background: The use of medical cannabis (MC) for palliation of symptoms is on the rise in cancer and rheumatological patients. Whether there is a potential for opioid dose reduction (ODR) and or quality of life improvements (QOL) is unclear. Methods: A retrospective cohort was evaluated to understand the pattern of care and QOL outcomes with MC use across rural multidisciplinary practices in New Mexico. MC use (> 1 mo.), EMR interrogation, urine toxicology screening were used to identify patients. QOL questionnaire included a graded pain scale. Morphine equivalent (ME) dose was used to estimate changes in opioid dose. ODR was defined as any reduction of baseline opioid dose. A chi-square was performed to evaluate associations.
Results: A total of 133 patients were identified between Jan 2017- May 2017. (M/F) 65/68; median age of 53 (range 20 - 84). Nineteen percent (25/133) had a cancer diagnosis. Pain score improved in 80 % of patients with cancer and in 75% (64/89) of non-cancer patients (x2 0.24 p = 0.62). ODR was achieved in 41% (54/133) of all patients on MC. Of these, 63% (34/54) had a 25% ODR and 37% (20/54) had 26% or more ODR (x2 12.8 p = 0.002). In cancer patients, a 25% ODR was achieved in 73% (x2 0.51 p = 0.771). All patients (15/15) using MC and high dose opioid (morphine equivalent ≥ 50 mg/day) had some ODR. Co-adjuvant NSAIDs with MC improved pain score in 67% of all cases vs 33% among non-NSAID cohort (x2 10.7 p = 0.001). ODR was achieved in 32% of patients with active depression vs 68% of patients without (x2 0.044 p = 0.83).
Conclusions: In this rural cohort, MC use led to ODR in 41% of all patients. Depression was a negative predictor of ODR. NSAID use facilitated ODR. It will be important to assess MC toxicity before considering this intervention. This study did not include toxicity data due to the retrospective nature of this study and its inherent limitations. Prospective data are needed to confirm these findings.
5. ‘Translational Investigation of the Therapeutic Potential of Cannabidiol (CBD): Toward a New Age’ | Front. Immunol., 21 September 2018 | https://doi.org/10.3389/fimmu.2018.02009
“Likewise, the lack of effective medicines to treat crack cocaine dependence is a clear indication of the need for further research in this field. In a collaborative animal study, we found that CBD protects against cocaine-induced seizures, possibly through activation of the mTOR pathway, with the concomitant reduction in glutamate release.”
Background: Among the many cannabinoids in the cannabis plant, cannabidiol (CBD) is a compound that does not produce the typical subjective effects of marijuana.
Objectives: The aim of the present review is to describe the main advances in the development of the experimental and clinical use of cannabidiol CBD in neuropsychiatry.
Methods: A non-systematic search was performed for studies dealing with therapeutic applications of CBD, especially performed by Brazilian researchers.
Results: CBD was shown to have anxiolytic, antipsychotic and neuroprotective properties. In addition, basic and clinical investigations on the effects of CBD have been carried out in the context of many other health conditions, including its potential use in epilepsy, substance abuse and dependence, schizophrenia, social phobia, post-traumatic stress, depression, bipolar disorder, sleep disorders, and Parkinson.
Discussion: CBD is an useful and promising molecule that may help patients with a number of clinical conditions. Controlled clinical trials with different neuropsychiatric populations that are currently under investigation should bring important answers in the near future and support the translation of research findings to clinical settings.
6. ‘Medicinal Properties of Cannabinoids, Terpenes, and Flavonoids in Cannabis, and Benefits in Migraine, Headache, and Pain: An Update on Current Evidence and Cannabis Science’ | First published: 27 August 2018 https://doi.org/10.1111/head.13345
A review found "accumulating evidence for various therapeutic benefits of cannabis/cannabinoids, especially in the treatment of pain, which may also apply to the treatment of migraine and headache" and that "there is also supporting evidence that cannabis may assist in opioid detoxification and weaning, thus making it a potential weapon in battling the opioid epidemic."
Abstract Background Comprehensive literature reviews of historical perspectives and evidence supporting cannabis/cannabinoids in the treatment of pain, including migraine and headache, with associated neurobiological mechanisms of pain modulation have been well described. Most of the existing literature reports on the cannabinoids Δ9‐tetrahydrocannabinol (THC) and cannabidiol (CBD), or cannabis in general. There are many cannabis strains that vary widely in the composition of cannabinoids, terpenes, flavonoids, and other compounds. These components work synergistically to produce wide variations in benefits, side effects, and strain characteristics. Knowledge of the individual medicinal properties of the cannabinoids, terpenes, and flavonoids is necessary to cross‐breed strains to obtain optimal standardized synergistic compositions. This will enable targeting individual symptoms and/or diseases, including migraine, headache, and pain.
Objective Review the medical literature for the use of cannabis/cannabinoids in the treatment of migraine, headache, facial pain, and other chronic pain syndromes, and for supporting evidence of a potential role in combating the opioid epidemic. Review the medical literature involving major and minor cannabinoids, primary and secondary terpenes, and flavonoids that underlie the synergistic entourage effects of cannabis. Summarize the individual medicinal benefits of these substances, including analgesic and anti‐inflammatory properties.
Conclusion There is accumulating evidence for various therapeutic benefits of cannabis/cannabinoids, especially in the treatment of pain, which may also apply to the treatment of migraine and headache. There is also supporting evidence that cannabis may assist in opioid detoxification and weaning, thus making it a potential weapon in battling the opioid epidemic. Cannabis science is a rapidly evolving medical sector and industry with increasingly regulated production standards. Further research is anticipated to optimize breeding of strain‐specific synergistic ratios of cannabinoids, terpenes, and other phytochemicals for predictable user effects, characteristics, and improved symptom and disease‐targeted therapies.
A study concluded that the "substantial reduction in opioid-related mortality associated with the implementation of medical cannabis laws can be explained by selection bias" because "states that legalized medical cannabis exhibit lower pre-existing mortality trends."
Abstract Mortality due to opioid overdoses has been growing rapidly in the U.S., with some states experiencing much steeper increases than others. Legalizing medical cannabis could reduce opioid-related mortality if potential opioid users substitute towards cannabis as a safer alternative. I show, however, that a substantial reduction in opioid-related mortality associated with the implementation of medical cannabis laws can be explained by selection bias. States that legalized medical cannabis exhibit lower pre-existing mortality trends. Accordingly, the mitigating effect of medical cannabis laws on opioid-related mortality vanishes when I include state-specific time trends in state-year-level difference-in-differences regressions.
8. ‘The Grass Might Be Greener: Medical Marijuana Patients Exhibit Altered Brain Activity and Improved Executive Function after 3 Months of Treatment’ | Front. Pharmacol., 17 January 2018 | https://doi.org/10.3389/fphar.2017.00983
Patients in a study of medical cannabis use "reported improvements in clinical state and health-related measures as well as notable decreases in prescription medication use, particularly opioids and benzodiazepines after 3 months of treatment."
Conclusion To our knowledge, this study represents the first neuroimaging investigation of patients using marijuana for medical purposes. Following 3 months of MMJ treatment, brain activation patterns appear more similar to those exhibited by healthy controls from previous studies than at pre-treatment. This finding provides strong evidence that MMJ treatment may normalize brain activity. Importantly, these changes were accompanied by improved task performance as well as positive changes in ratings of clinical state, impulsivity, sleep, and quality of life. Further, patients reported notable decreases in their use of conventional medications, including opioids. In light of the national opioid epidemic, these data clearly underscore the need to expand and extend this study to determine if a reduction in opioid use persists with continued MMJ treatment. Results from the current study raise the possibility that the observed improvements in cognition and related changes in functional activation patterns may be related to direct and/or indirect effects of cannabinoids, specifically within an adult population beyond the stages of critical neuromaturation. Patients utilizing MMJ appear to use products with different cannabinoid profiles (i.e., high CBD) relative to recreational users, which is also likely to impact cognitive function. Observed changes may also be related to secondary or more indirect effects, including the reduction of clinical symptoms, improved sleep, and decreased use of conventional medications. Additional studies using both observational and clinical trial models to examine the impact of actual MMJ products used by patients are needed to clarify the underlying neural mechanisms associated with clinical and behavioral changes that accompany MMJ treatment.
9. ‘Association Between US State Medical Cannabis Laws and Opioid Prescribing in the Medicare Part D Population’ | May 2018 | JAMA Intern Med. 2018;178(5):667-672. doi:10.1001/jamainternmed.2018.0266
Key Points Question: What is the association between US state implementation of medical cannabis laws and opioid prescribing under Medicare Part D?
Findings: This longitudinal analysis of Medicare Part D found that prescriptions filled for all opioids decreased by 2.11 million daily doses per year from an average of 23.08 million daily doses per year when a state instituted any medical cannabis law. Prescriptions for all opioids decreased by 3.742 million daily doses per year when medical cannabis dispensaries opened.
Meaning: Medical cannabis policies may be one mechanism that can encourage lower prescription opioid use and serve as a harm abatement tool in the opioid crisis.
Abstract Importance: Opioid-related mortality increased by 15.6% from 2014 to 2015 and increased almost 320% between 2000 and 2015. Recent research finds that the use of all pain medications (opioid and nonopioid collectively) decreases in Medicare Part D and Medicaid populations when states approve medical cannabis laws (MCLs). The association between MCLs and opioid prescriptions is not well understood.
Objective: To examine the association between prescribing patterns for opioids in Medicare Part D and the implementation of state MCLs.
Design, Setting, and Participants: Longitudinal analysis of the daily doses of opioids filled in Medicare Part D for all opioids as a group and for categories of opioids by state and state-level MCLs from 2010 through 2015. Separate models were estimated first for whether the state had implemented any MCL and second for whether a state had implemented either a dispensary-based or a home cultivation only–based MCL.
Main Outcomes and Measures: The primary outcome measure was the total number of daily opioid doses prescribed (in millions) in each US state for all opioids. The secondary analysis examined the association between MCLs separately by opioid class.
Results: From 2010 to 2015 there were 23.08 million daily doses of any opioid dispensed per year in the average state under Medicare Part D. Multiple regression analysis results found that patients filled fewer daily doses of any opioid in states with an MCL. The associations between MCLs and any opioid prescribing were statistically significant when we took the type of MCL into account: states with active dispensaries saw 3.742 million fewer daily doses filled (95% CI, −6.289 to −1.194); states with home cultivation only MCLs saw 1.792 million fewer filled daily doses (95% CI, −3.532 to −0.052). Results varied by type of opioid, with statistically significant estimated negative associations observed for hydrocodone and morphine. Hydrocodone use decreased by 2.320 million daily doses (or 17.4%) filled with dispensary-based MCLs (95% CI, −3.782 to −0.859; P = .002) and decreased by 1.256 million daily doses (or 9.4%) filled with home-cultivation–only-based MCLs (95% CI, −2.319 to −0.193; P = .02). Morphine use decreased by 0.361 million daily doses (or 20.7%) filled with dispensary-based MCLs (95% CI, −0.718 to −0.005; P = .047).
Conclusions and Relevance: Medical cannabis laws are associated with significant reductions in opioid prescribing in the Medicare Part D population. This finding was particularly strong in states that permit dispensaries, and for reductions in hydrocodone and morphine prescriptions.
INTRODUCTION: Prescription drug overdoses are the leading cause of accidental death in the United States. Alternatives to opioids for the treatment of pain are necessary to address the issue. Cannabis can be an effective treatment of pain, greatly reduces the chance of dependence, and eliminates the risk of fatal overdose compared to opioid-based medications. Medical cannabis patients report that cannabis is just as effective, if not more, than opioid-based medications for pain.
MATERIALS AND METHODS: The current study examined the use of cannabis as a substitute for opioid-based pain medication by collecting survey data from 2897 medical cannabis patients.
CONCLUSION: Future research should track clinical outcomes where cannabis is offered as a viable substitute for pain treatment examine the outcomes of using cannabis as a medication assisted treatment for opioid dependence.
Research For Cannabinoid Therapies for the Substance Abuse Disorder 1. ‘Alcohol Abuse, Dependence, Tolerance, and Withdrawal’
Alcoholism is an addiction one has to the consumption of alcoholic liquor or the mental illness and compulsive behavior resulting from alcohol dependency.
Alcohol dependence (i.e. alcoholism) may result from alcohol abuse (i.e. use of alcohol in a way that negatively impacts one’s actions/life), and is characterized by a feeling that one needs to consume alcohol in order to function normally, with a decreased ability to stop drinking even if the desire to do so exists. Those with alcohol dependence develop tolerance to alcohol, meaning that they need to consume more and more over time in order to feel the same effect they experienced the first time they drank. If alcohol consumption then stops, especially abruptly, individuals with alcohol dependence will experience symptoms of alcohol withdrawal.
Mild alcohol withdrawal is characterized by signs and symptoms including anxiety, development of tremors/shakiness, depression, irritability, fatigue, palpitations, etc., while severe alcohol withdrawal is characterized by more serious events, such as the onset of seizures and delirium tremens (with symptoms including a confused state, fever, tremors/shakiness, seizures, changes in mental functioning, irritability, hallucinations), which can lead to death in 1-5% of cases.
Even if a person who is alcohol-dependent wants to stop drinking, the negative impact of withdrawal will often prevent them from doing so (i.e. they may continue to drink to avoid the associated undesirable feelings).
Of the 38 million adults in the United states who drink too much, approximately 17 million of them have alcohol abuse disorders. Alcohol abuse is the 3rd leading cause of preventable death and results in costs totaling over $200 billion each year. Due to the huge impact alcohol abuse has on people, their families, and society, and to the fact that alcohol withdrawal is a major impediment to stopping alcohol abuse/overuse, its management is paramount to helping people overcome alcohol dependence.
Study Results
Using PET scans (which help us to visualize the functioning of organs and tissues) to measure activity/availability of CB1 receptors (a cannabinoid receptor found most commonly in the brain and spinal cord), authors of a study published in The Journal of Neuroscience in February 2014 found that cannabinoid signaling varies in the brains of alcohol non-users, non-dependent alcohol users, and dependent alcohol users.
Researchers found that in the brains of social, non-dependent drinkers (i.e. “non-alcoholic” drinkers, n=20), activity/availability of CB1 receptors was significantly increased after administration of ethanol (i.e. alcohol) into the bloodstream.
On the other hand, activity/availability of CB1 receptors was significantly decreased in dependent users (i.e. “alcoholics”, n=26) after long-term, heavy use of alcohol, even after 1 month of abstinence (no alcohol use). After long-term, heavy use, activity/availability was especially decreased in the areas of the cerebellum (part of the brain involved in coordinating movements, producing fine movements, maintaining posture and balance, etc.) and the parieto-occipital cortex (area of the brain which may be involved in planning processes). After abstinence, additional areas of decreased activity/availability of CB1 receptors were the ventral striatum (a part of the brain activated when a reward/pleasurable feeling is perceived) and the mesial temporal lobe (an area whose damage is sometimes associated with epileptic seizures). Conclusion
CB1 receptor stimulation is involved with subjectively feeling reward/pleasure. However, if the receptors are overstimulated, as by long-term, heavy use of alcohol, their activity/availability will decrease. During a period of abstinence from alcohol, this decreased stimulation may lead to an increased craving for alcohol, in order to re-establish the positive feelings associated with its use. Additionally, during the early phases of abstinence, neurons become hyperexcitable (i.e. overactivated), which can lead to their damage and death.
Therefore, for alcohol-dependent individuals attempting to reduce or eliminate their alcohol use, treatments aimed at increasing signaling of cannabinoid receptors in the brain [e.g. (1) cannabinoid therapies (such as targeted, isolated/synthetic CB1 receptor “stimulators”, or potentially whole-plant use if deemed appropriate by and closely monitored by a healthcare provider) or (2) therapies that upregulate CB1 receptors], may be useful for the following reasons:
Since cannabinoids may act as neuroprotective agents (with the potential to reduce hyperexcitability and prevent brain cell damage), cannabinoid therapies may directly prevent harm to the brain caused by withdrawal.
Cannabinoid therapy use, in combination with alcohol abstinence, may be helpful in the treatment of alcohol dependence and withdrawal by assisting in the prevention of alcohol cravings.
2. ‘Cannabis as a Substitute for Alcohol: A Harm-Reduction Approach’ by Tod H. Mikuriya
ABSTRACT. Ninety-two Northern Californians who use cannabis as an alternative to alcohol obtained letters of approval from the author. Their records were reviewed to determine characteristics of the cohort and efficacy of the treatment, which was defined as reduced harm to the patient. All patients reported benefit, indicating that for at least a subset of alcoholics, cannabis use is associated with reduced drinking. The cost of alcoholism to individual patients and society at large warrants testing of the cannabis-substitution approach and study of the drug-of-choice phenomenon.
It is no secret that alcohol consumption can negatively affect one’s liver. This is because it can cause an excess of fats and lipids and additional oxidative stress (i.e. damage caused by free radicals).
With that said, a recent study published in Free Radical Biology and Medicine offers an interesting preventive measure. Funded by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) and the National Institutes of Health (NIH), it suggests that cannabidiol (CBD) could help protect the liver from alcohol-induced damage.
Researchers Prevent Alcohol-Induced Liver Damage With CBD.
As we know, cannabidiol (CBD) may have antioxidant effects. Couple that with the constituent’s lack of psychoactivity, and it makes sense why the team of researchers from China and Mount Sinai School of Medicine in New York chose to investigate its ability to counter alcohol-induced oxidative stress in the liver.
In doing so, they injected mice with ethanol twice a day for five days. This was intended to model the impact of binge drinking on one’s liver. Prior to this, a group of the mice were administered cannabidiol (CBD) as a preventive measure.
“The study’s results seem to confirm that cannabidiol (CBD) protects the liver from steatosis – the accumulation of fats and lipids.”
Sure enough, the study’s results showed that cannabidiol (CBD) may protect the liver from steatosis – the accumulation of fats and lipids. The researchers suggested that this was potentially the result of cannabidiol inhibition of oxidative stress and activation of pathways associated with fat accumulation.
The accumulation of fat in the liver can lead to much more serious problems like cirrhosis of the liver (i.e. scarring of the liver that may lead to liver failure) if it gets out of hand. With that said, there is no easy way to go about “curing” the disease once it occurs, so taking a preventive approach is best. Although increased research may strengthen the theory that cannabidiol (CBD) administration helps to prevent alcohol-induced liver damage, cannabidiol is not an approved or definitively effective preventive treatment at the present time.
4. ‘Study: CBD-Based Topicals May Aid In Alcoholism Treatment
What Is CBD’s Effect On Brain Degradation?’
According to the National Institute of Alcohol Abuse and Alcoholism (NIAAA), alcohol can be linked to neurodegradation (i.e. breakdown of neurons, which are brain cells that communicate with each other to transmit signals) among other effects. Due to the fact that cannabidiol (CBD) has been found to potentially have neuroprotectiveeffects, a study published last week in Pharmocology Biochemisty & Behavior aimed to explore the effect of cannabidiol topicals on alcohol-induced brain degradation.
It is important to understand the causes of, and ways to prevent, degradation associated with excessive alcohol use, because some believe that the behavioral and cognitive deficits it causes may be linked to alcoholisms high relapse rate (i.e. many people with alcohol dependence who stop drinking eventually start drinking again). The researchers, who were from the University of Kentucky, AllTranz Inc., and the University of Maryland, hoped to compare cannabidiol topicals with a direct injection of CBD.
5. ‘Medical Cannabis as a Recovery Treatment’
Since cannabis has earned an undeserved negative reputation in many quarters, it is often difficult to determine what is fact and what is politics when talking about medical marijuana. However, the following three studies pointed to definite possibilities of using cannabis to overcome dependence on more harmful drugs and alcoholism:
A 2009 study performed by the Laboratory for Physiopathology of Diseases of the Central Nervous System found that injections of THC, the primary active chemical in cannabis, helped eliminate dependence on opiates such as morphine and heroin in test animals.
A survey compiling self-reported addiction treatment and relapse rates among substance users, “Cannabis as a Substitute for Alcohol and Other Drugs” that was published in the Harm Reduction Journal, found that respondents used cannabis to curb their alcohol cravings, as an alternative to previous use of prescription drugs, and even as a substitute for more potent drugs such as cocaine. Tellingly, 57.4% of respondents chose to use cannabis because it provided better symptom management as well.
Another study published in the Harm Reduction Journal, “Long term cannabis users seeking medical cannabis in California,” found that medical cannabis users were much less likely to use more potent drugs, and even reported less tobacco use than non-cannabis users.
Why Use Cannabis as a Recovery Treatment?
It’s clear that more effective addiction recovery treatment is needed in our country. According to the National Institute on Drug Abuse, depending on the addiction, up to half of individuals who begin an addiction treatment program relapse within six months. As more states move to legalize medical marijuana, it is becoming easier for scientists, doctors, and researchers to point to the benefits of cannabis as a treatment for pain relief and symptom management for many diseases. Benefits now known to the scientific community include:
Medical cannabis patients are able to function more fully in daily activities and work, unlike with many prescription opiates for symptom relief.
Medical cannabis patients report fewer unpleasant side effects with marijuana than with many traditional and stronger drug treatments.
Medical cannabis patients achieve more effective symptom relief using marijuana than with other alternatives.
Since withdrawal from alcohol and serious drug use often prompts the same symptoms as other medical conditions that cannabis is used to treat (anxiety, depression, pain, nausea, and sleeplessness,) it is logical that responsible use of marijuana could also help with addiction recovery.
6. ‘Cannabis Shown To Ease Symptoms During Opiate Withdrawal’
According to a recent study, cannabis use may help relieve withdrawal symptoms during Methadone treatment. The study that was performed at Thomas Jefferson University and recently published online shows the cannabinoid system may have a place in future substance abuse treatment. This Pennsylvania-based university was the home for observing 91 patients undergoing Methadone treatment.
Methadone is common form of treatment for opiate dependence. It can be effective, but it has a number of negative side effects.
There are quite a few reported side effects of Methadone treatment, such as: anxiety, insomnia, nausea, loss of appetite, and even psychological dependence.
These are only a few of the reported side effects and there are likely more that go unreported. Perhaps the scariest side effect is the psychological dependence. An opiate-dependent patient is putting their trust into a treat to break their vicious dependence. Sadly, instead of curing the patient of their dependence they start to need the treatment as much as they did the original opiates.
Cannabis Use Reduced Opiate Withdrawal Symptoms
According to the Thomas Jefferson University study, cannabis use before and during treatment decreased the patients score on the Clinical Opiate Withdrawal Scale (COWS). This is a scale used to objectively determine withdrawal symptoms in opiate-dependent patients. The lower scores indicate that cannabis plays a role in reducing the symptoms of opiate withdrawal.
“The present findings may point to novel interventions to be employed during treatment for opiate dependence that specifically target cannabinoid-opioid system interactions” – Thomas Jefferson University, Philadelphia.
This study suggests that cannabis may play a role in increasing the success of Methadone treatment. The reason for this is that is lowers the amount of withdrawal symptoms patients experience.
As discussed earlier, common symptoms of opiate withdrawal include anxiety, muscle aches, insomnia, abdominal cramps, and nausea. Medical cannabis is already being used to successfully treat each of these symptoms with little to no known side effects. “Cannabis does not have the physical addictive components that opiates do,” says Shelley Stormo, a clinical psychologist at Gosnold. “It does not have the propensity, as opiates do, for overdoses. There’s no documented death by overdose of cannabis.”
We are in the throes of an opioid abuse crisis and are desperately searching for an answer. It’s time we acknowledge the solution that’s right in front of us and make this life-saving treatment available for those dependent on opioids. Cannabis has been proven to relieve chronic pain while reducing and replacing the use of opioids. It also relieves the symptoms of opioid withdrawal and decreases opioid craving. There is no toxic or lethal overdose of cannabis, and thousands of patients are already effectively using cannabis to replace opioids and other addictive substances.
8. ‘Medical Cannabis As An Exit Drug for Addiction’
"Research suggests that people are using cannabis as an exit drug to reduce the use of substances that are potentially more harmful, such as opioid pain medication." Says a lead investigator on addiction, Zach Walsh, a professor of psychology at University of British Columbia.
Medical cannabis is legal in 28 states and the District of Columbia. Still, the DEA classifies cannabis as a Schedule I controlled substance, the same category as heroin. US Patent No. 6630507, is held by the United States Department of Health and Human Services. The Patent covers the use of cannabinoids for treating a wide range of diseases. Yet under U.S. federal law, cannabis is defined as having no medical use. So it might come as a surprise to hear that the government owns a patent on cannabis as a medicine. The patent (US6630507) is titled “Cannabinoids as antioxidants and neuroprotectants". It was awarded to the Department of Health and Human Services (HHS) in October 2003. It was filed in 1999, by a group of scientists from the National Institute of Mental Health (NIMH), also part of the National Institutes of Health.
9. ‘Cannabidiol inhibits the reward-facilitating effect of morphine: involvement of 5-HT1A receptors in the dorsal raphe nucleus’
Unlike hospice, long-term drug safety is an important issue in palliative medicine. Opioids may produce significant morbidity. Cannabis is a safer alternative with broad applicability for palliative care. Yet the Drug Enforcement Agency (DEA) classifies cannabis as Schedule I (dangerous, without medical uses). Dronabinol, a Schedule III prescription drug, is 100% tetrahydrocannabinol (THC), the most psychoactive ingredient in cannabis. Cannabis contains 20% THC or less but has other therapeutic cannabinoids, all working together to produce therapeutic effects. As palliative medicine grows, so does the need to reclassify cannabis. This article provides an evidence-based overview and comparison of cannabis and opioids. Using this foundation, an argument is made for reclassifying cannabis in the context of improving palliative care and reducing opioid-related morbidity.
Am J Hosp Palliat Care. 2011 Aug;28(5):297-303. doi: 10.1177/1049909111402318. Epub 2011 Mar 28.
10. ‘Cannabidiol as an Intervention for Addictive Behaviors: A Systematic Review of the Evidence’ | Prud’homme et al. Cannabidiol as an Intervention for Addictive Behaviors: A Systematic Review of the Evidence. Substance Abuse: Research and Treatment 2015:9 33–38 doi: 10.4137/SART.S25081. | https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4444130/pdf/sart-9-2015-033.pdf
Abstract: Drug addiction is a chronically relapsing disorder characterized by the compulsive desire to use drugs and a loss of control over consumption. Cannabidiol (CBD), the second most abundant component of cannabis, is thought to modulate various neuronal circuits involved in drug addiction. The goal of this systematic review is to summarize the available preclinical and clinical data on the impact of CBD on addictive behaviors. MEDLINE and PubMed were searched for English and French language articles published before 2015. In all, 14 studies were found, 9 of which were conducted on animals and the remaining 5 on humans. A limited number of preclinical studies suggest that CBD may have therapeutic properties on opioid, cocaine, and psychostimulant addiction, and some preliminary data suggest that it may be beneficial in cannabis and tobacco addiction in humans. Further studies are clearly necessary to fully evaluate the potential of CBD as an intervention for addictive disorders.
Abstract The role of the endocannabinoid system in nicotine addiction is being increasingly acknowledged. We conducted a pilot, randomised double blind placebo controlled study set out to assess the impact of the ad-hoc use of cannabidiol (CBD) in smokers who wished to stop smoking. 24 smokers were randomised to receive an inhaler of CBD (n=12) or placebo (n=12) for one week, they were instructed to use the inhaler when they felt the urge to smoke. Over the treatment week, placebo treated smokers showed no differences in number of cigarettes smoked. In contrast, those treated with CBD significantly reduced the number of cigarettes smoked by ~40% during treatment. Results also indicated some maintenance of this effect at follow-up. These preliminary data, combined with the strong preclinical rationale for use of this compound, suggest CBD to be a potential treatment for nicotine addiction that warrants further exploration.
Abstract BACKGROUND AND PURPOSE: Abrupt discontinuation of nicotine, the main psychoactive component in tobacco, induces a withdrawal syndrome in nicotine-dependent animals, consisting of somatic and affective signs, avoidance of which contributes to drug maintenance. While blockade of fatty acid amide hydrolase, the primary catabolic enzyme of the endocannabinoid arachidonoylethanolamine (anandamide), exacerbates withdrawal responses in nicotine-dependent mice, the role of monoacylglycerol lipase (MAGL), the main hydrolytic enzyme of a second endocannabinoid 2-arachidonylglycerol (2-AG), in nicotine withdrawal remains unexplored. EXPERIMENTAL APPROACH: To evaluate the role of MAGL enzyme inhibition in nicotine withdrawal, we initially performed a genetic correlation approach using the BXD recombinant inbred mouse panel. We then assessed nicotine withdrawal intensity in the mouse after treatment with the selective MAGL inhibitor, JZL184, and after genetic deletion of the enzyme. Lastly, we assessed the association between genotypes and smoking withdrawal phenotypes in two human data sets. KEY RESULTS: BXD mice displayed significant positive correlations between basal MAGL mRNA expression and nicotine withdrawal responses, consistent with the idea that increased 2-AG brain levels may attenuate withdrawal responses. Strikingly, the MAGL inhibitor, JZL184, dose-dependently reduced somatic and aversive withdrawal signs, which was blocked by rimonabant, indicating a CB1 receptor-dependent mechanism. MAGL-knockout mice also showed attenuated nicotine withdrawal. Lastly, genetic analyses in humans revealed associations of the MAGL gene with smoking withdrawal in humans. CONCLUSIONS AND IMPLICATIONS: Overall, our findings suggest that MAGL inhibition maybe a promising target for treatment of nicotine dependence.
“Because cannabis did not lead to physical dependence, it was found to be superior to the opiates for a number of therapeutic purposes. Birch, in 1889, reported success in treating opiate and chloral addiction with cannabis, and Mattison in 1891 recommended its use to the young physician, comparing it favorably with the opiates.”
Mikuriya found Cannabis to be non habit forming as well…
“.. . there is positively no evidence to indicate the abuse of cannabis as a medicinal agent or to show that its medicinal use is leading to the development of cannabis addiction. Cannabis at the present time is slightly used for medicinal purposes, but it would seem worthwhile to maintain its status as a medicinal agent for such purposes as it now has. There is a possibility that a re-study of the drug by modern means may show other advantages to be derived from its medicinal use.”(Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1503422/pdf/califmed00019-0036.pdf)
“…in spite of the legends, no case of physical, mental or moral degeneration has ever been traced exclusively to marijuana… Because of its non-habit-forming character, doctors have recently been experimenting with the drug as an aid in curing opium addiction.” (Link:http://content.time.com/time/magazine/article/0,9171,777874-2,00.html)
Go to any responsible detox facility for alcohol and you will immediately be put on highly addictive benzodiazepines. Go to detox for heroin or oxycontin and your opiate of choice will be replaced by an opioid like suboxone. Most of our treatment involves putting people on different drugs but we just call them medications instead to soften the idea. Using marijuana to treat addiction may be the first step in shifting the treatment landscape towards the use of natural plant medicines to promote recovery.
Yes, using plant medicines within an integrated treatment model is using a substance to treat substance use. But, that’s what we already do, and right now we do it with drugs that are far more damaging and addictive. The risk of addiction to plant medicines is minimal. Yet, the go-to drugs in alcohol detox (benzodiazepines) and opioid replacement therapy (methadone, suboxone) are powerfully addictive and withdrawal from them can be highly uncomfortable or even fatal in the case of benzodiazepines. Using ibogaine or psilocybin to interrupt addiction and cannabis as a bridge to a new lifestyle may sound like the ravings of madmen now, but it may just be the norm in 50 years.
While we would like to imagine that everyone who’s addicted to any substance could successfully get off substances all together, we recognize that that’s not practical. Abstinence just doesn’t work for everyone. So instead of focusing on abstinence, we take a safer substance and use it to replace a more harmful substance. This is the practice of harm reduction.
Rules, Regulations, & Policy Solution for this Petition: Requesting The Inclusion Of A New Medical Condition: Substance Abuse Disorder; To Include: Alcohol Use Disorder (AUD), Tobacco Use Disorder, Stimulant Use Disorder, Hallucinogen Use Disorder, and Opioid Use Disorder
Approval of this Petition will Save Many Lives in New Mexico...
The approval of this Petition: Requesting The Inclusion Of A New Medical Condition: Substance Abuse Disorder; To Include: Alcohol Use Disorder (AUD), Tobacco Use Disorder, Stimulant Use Disorder, Hallucinogen Use Disorder, and Opioid Use Disorder- that is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
The approval of this petition will fulfill the intent of the law and uphold the integrity and spirit of the Lynn and Erin Compassionate Use Act, 2007.
Fulfilling both;“ Section 2. PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments”
And of section 6. ADVISORY BOARD CREATED--DUTIES: The advisory board shall:
A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis.” New Mexico’s medical cannabis history started in 1978. After public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis...the first law.
New Research Added to Petition for the December 10th MCAB Hearing:
1. Vast Majority of Substance Abuse Professionals Support Legalizing Medical Cannabis
A study found that the vast majority of substance abuse professionals support legalizing medical cannabis and believe that cannabis is safe when used responsibly for medical purposes.
A new study examining the attitudes of addiction treatment professionals towards medical marijuana suggests that the majority support legalization and feel it is safe. According to reports on the study, 71 percent of addiction clinicians believe marijuana should be legalized for medical use and 70 percent stated marijuana is safe when used responsibly for medical purposes.
Researchers from Towson University in Maryland conducted the study to gain more specific views on medical marijuana from substance abuse health professionals. They surveyed 966 addiction clinicians, primarily from the midwest and east coast. Participants were identified through state licensing and certification boards.
The surveys included 22 statements and offered participants the chance to rate how much they agreed or disagreed. Participants were also asked to reveal their personal encounters with marijuana.
According to the study, 74 percent reported having used marijuana, 73 percent reported knowing a medical cannabis patient, and 61 percent reported knowing patients with addiction issues who had used marijuana in recovery. Findings also showed that younger participants and those who practiced on the east coast viewed medical marijuana more favorably.
In conclusion, the researchers noted more research is needed to gain a better understanding of the mixed attitudes of addiction clinicians towards medical cannabis.
“These mixed attitudes may actually reflect a healthy skepticism,” researchers concluded. “That is, if the current trends continue, addictions treatment professionals may be poised to both accept medical marijuana legalization and to handle any associated negative consequences.”
More than half of the participants were women with masters or doctoral degrees. The average participant’s age was 46.
ABSTRACT Background: Research on health professional’s attitudes toward medical marijuana have failed to include addictions treatment professionals. The current study attempted to address this gap in the literature.
Methods: Study participants were recruited by e-mail using mailing lists supplied by multiple state licensing/certification boards and through snowball sampling. Participants completed a 22-item survey addressing attitudes toward medical and recreational marijuana. The 13 items relating to medical marijuana were analyzed.
Results: Our sample (N = 966) was largely female (69.1%) with a Masters’ or Doctoral degree (80%) and a mean age of 46.5 (SD = 12.8). Participants were mostly split between the mid-west and east coast. Overall, participants held mixed views toward medical marijuana. For example, 71.3% of the sample supported legalization of marijuana for medical purposes and yet 63.6% believed that medical marijuana is often abused.
Conclusions: More research is needed to develop a more nuanced understanding of substance use treatment provider’s mixed attitudes toward medical marijuana legalization.
2. Cannabis Use to Treat Addiction In the study examining addiction clinicians’ views on marijuana, findings show that many of the health professionals believe cannabis could be helpful for symptoms associated with addiction. Those symptoms include anxiety and trouble sleeping, two common qualifications for many state medical marijuana programs.
Other research has found similar results when it comes to cannabis as an aid in treating substance addiction. A recent study published in the journal Addiction found that addiction treatment patients who used cannabis daily were more likely to stick with their treatment compared to those who did not use cannabis.
Researchers from the British Columbia Centre on Substance Use (BCCSU) and the University of British Columbia (UBC) interviewed 820 people enrolled in opioid agonist treatment (OAT) programs over a 20-year period, between December 1996 and March 2016.
OAT is a treatment regimen involving taking opioid agonists methadone or buprenorphine to prevent withdrawal and reduce cravings for opioid drugs.
The researchers found that everyday cannabis use is associated with greater retention rates. The participants who reported using marijuana daily were approximately 21 percent more likely to still be in the treatment after six months than non-using participants.
“The therapeutic benefits of cannabis are only just beginning to be understood,” said Dr. M-J Milloy, senior author and research scientist at BCCSU. “This research suggests that cannabis could have a stabilizing impact for many patients on treatment, while also reducing the risk of overdose. Further examination of its therapeutic value and clinical application is clearly needed.”
Cannabis use could be a “gateway” out of more harmful substance use, according to new research (published on March 29, 2018)
Cannabis use makes it less likely some people who use drugs will start injecting drugs, according to research from the British Columbia Centre on Substance Use (BCCSU).
Research published in Drug and Alcohol Review (March 2018, Volume 37, Issue 3) found street-involved youth who used cannabis were less likely to begin using drugs via injection. The study followed 481 participants who were injection-naïve at the time of recruitment. From study enrolment, the median time to injection initiation was 13 months. However, daily cannabis use was associated with a 34% decrease in the rate of injection initiation.
The average age of injection initiation is between 19 and 23 years, and street-involved youth are known to be at elevated risk of initiating injection drug use and engaging in high-risk drug practices such as needle sharing. People who use injection drugs also face increased risk of infection with HIV and hepatitis C, accidental overdose, stigmatization, and criminalization.
“One common perception about cannabis is that it’s a so-called gateway drug to other, higher risk drug use. However, our study found the opposite,” says senior author Dr. M-J Milloy, research scientist at BCCSU and Assistant Professor at the University of British Columbia.
Previous research from the BCCSU supports the findings in this latest study. In an article published last year in Harm Reduction Journal, researchers found that cannabis use may aid in quitting injection drug use. Another study published last year in International Journal of Drug Policy described how youth attempt to reduce harms stemming from addiction, including using cannabis to reduce or eliminate use of drugs they considered more harmful, such as crystal meth, crack cocaine, and opioids.
“These findings suggest the risks and possible benefits of cannabis use – particularly among high-risk youth – are not fully understood,” says Dr. Milloy. “With the impending legalization of cannabis in Canada, future studies into the impact of cannabis use on high-risk drug behaviours are needed.”
Data for the studies were derived from the At-Risk Youth Study (ARYS), a prospective cohort of street-involved youth in Vancouver aged 14-26 years, and looked at the results of interviews conducted between September 2005 and May 2015.
3. B.C. researchers find that cannabis could help reduce crack cocaine use published on May 16, 2017
Research presented by BC Centre on Substance Use scientists at Harm Reduction International Conference in Montreal offers possible treatment for harmful crack cocaine use
Vancouver, B.C. (May 16, 2017) – Using cannabis might be an effective strategy for people seeking to control their use of crack cocaine, according to new research from scientists at the BC Centre on Substance Use (BCCSU).
Scientists examined the crack use histories of 122 people who use drugs in Vancouver’s Downtown Eastside and Downtown South neighbourhoods and observed reductions in the frequency of crack use following periods in which they reported using cannabis to control their crack use. The research was presented today at the 2017 Harm Reduction International (HRI) Conference in Montreal.
“Crack cocaine, whether it’s injected or inhaled, is associated with an array of negative health consequences, including cuts and burns from unsafe pipes and the transmission of infectious diseases such as HIV and hepatitis C,” said Dr. Eugenia Socias, a physician and postdoctoral fellow at BCCSU and first author of the study who presented the research at the HRI Conference. “We found that intentional cannabis use preceded declines in crack use among crack cocaine users who pursued self-medication with cannabis.”
According to recent estimates, there are between 14 and 21 million current users of cocaine worldwide, of whom approximately seven million have a cocaine use disorder. A substantial proportion of cocaine use is thought to occur in the form of crack cocaine, particularly among marginalized populations in urban settings in North and South America. Risks associated with crack cocaine include accidental overdose and transmission of infectious diseases, such as hepatitis and HIV. There exist no effective pharmaceutical therapies for crack cocaine use.
The BCCSU’s research is the largest longitudinal study to demonstrate the potential role of cannabis use as a reduction or substitution strategy for crack cocaine use. The findings are in line with smaller case ad qualitative studies in Jamaica and Brazil. For instance, a study conducted in Brazil – which has struggled with a crack cocaine epidemic and is the largest consumer of crack cocaine in the world – followed 25 treatment-seeking individuals with crack use disorders who reported using cannabis to reduce cocaine-related craving symptoms. Over a nine-month follow-up period, the majority (68%) stopped using crack.
“Problematic crack cocaine use causes immense human suffering globally,” said Dr. M-J Milloy, a research scientist at the BCCSU and senior author of the paper. “In the absence of effective therapies for crack dependence, our findings provide a foundation on which to explore the potential of cannabis to treat problematic substance use. The federal government’s plans to legalize cannabis represents a tremendous opportunity to support research in this area and we plan to further investigate whether cannabis could contribute to reducing the harms of crack cocaine use among marginalized drug users.” [https://www.bccsu.ca/news-release/b-c-researchers-find-that-cannabis-could-help-reduce-crack-cocaine-use/]
4. Reduction of Benzodiazepine Use in Patients Prescribed Medical Cannabis Abstract Background: Benzodiazepines are a class of medication with sedative properties, commonly used for anxiety and other neurological conditions. These medications are associated with several well-known adverse effects. This observational study aims to investigate the reduction of benzodiazepine use in patients using prescribed medical cannabis.
Methods: A retrospective analysis was performed on a cohort of 146 medical cannabis patients (average age 47 years, 61% female, 54% reporting prior use of cannabis) who reported benzodiazepine use at initiation of cannabis therapy. These data are a part of a database gathered by a medical cannabis clinic (Canabo Medical). Descriptive statistics were used to quantify associations of the proportion of benzodiazepine use with time on medical cannabis therapy.
Results: After completing an average 2-month prescription course of medical cannabis, 30.1% of patients had discontinued benzodiazepines. At a follow-up after two prescriptions, 65 total patients (44.5%) had discontinued benzodiazepines. At the final follow-up period after three medical cannabis prescription courses, 66 total patients (45.2%) had discontinued benzodiazepine use, showing a stable cessation rate over an average of 6 months.
Conclusion: Within a cohort of 146 patients initiated on medical cannabis therapy, 45.2% patients successfully discontinued their pre-existing benzodiazepine therapy. This observation merits further investigation into the risks and benefits of the therapeutic use of medical cannabis and its role relating to benzodiazepine use.
Narrative: Researchers discovered that nearly half of patients discontinued their use of anti-anxiety meds after starting with medical cannabis.
Findings in a new study published in Cannabis and Cannabinoid Research suggest that cannabis can be used as an effective alternative to traditional anti-anxiety medications.
A team of Canadian researchers assessed the relationship between cannabis and benzodiazepines, a class of drugs that work in the central nervous system and are primarily used for treating anxiety. Common benzodiazepines include Xanax, Ativan, and Valium.
Using a cohort of 146 patients enrolled in Canada’s medical marijuana program, the researchers discovered a large portion of patients had substituted cannabis for their anti-anxiety drugs.
“Patients initiated on medical cannabis therapy showed significant benzodiazepine discontinuation rates after their first follow-up visit to their medical cannabis provider, and continued to show discontinuation rates thereafter,” the study concluded.
Specifically, the cannabis in place of benzodiazepines study found that 30 percent of patients reported discontinuing their use of benzodiazepines within two months of starting medical cannabis treatment. By the six-month check-in with their cannabis doctor, 45 percent of patients stopped anti-anxiety medication use.
The participating patients, once initiating medical marijuana use, also reported decreased daily distress from their medical conditions.
While doctors commonly prescribe benzodiazepines to treating anxiety, the drugs also associated with potentially serious side effects and risks. According to the United States Centers for Disease Control and Prevention, the drug was attributed to over 11,500 fatal overdoses in 2017. Nobody has ever reportedly died of a cannabis overdose.
“The study results are encouraging, and this work is concurrent with growing public interest in a rapidly developing Canadian cannabis market,” said lead author of the cannabis in place of benzodiazepines study, Chad Purcell.
“We are advising the public to observe caution. The results do not suggest that cannabis should be used as an alternative to conventional therapies. Our purpose is inspiring others to advance current cannabis understanding as we collect stronger efficacy and safety data that will lead to responsible policy and recommended practices for use.”
The new cannabis in place of benzodiazepines study, “Reduction of Benzodiazepine Use in Patients Prescribed Medical Cannabis,” is available to access in full for free through the journal Cannabis and Cannabinoid Research. [https://www.liebertpub.com/doi/full/10.1089/can.2018.0020]
5. A pair of studies link medical cannabis to reduced risk of alcoholic-induced pancreatitis and alcoholic gastritis
The two studies showed heavy drinkers who concurrently use cannabis are at a reduced risk of alcoholic-induced pancreatitis and alcoholic gastritis.
Those who partake in heavy alcohol drinking and also use cannabis are at a reduced risk of developing pancreatic gastritis and alcoholic gastritis compared to heavy drinkers who don’t use cannabis, according to a pair of new studies published in the journal Alcoholism, Clinical and Experimental Research.
For the two studies, a team of researchers from the United States and Canada accessed nationwide samples to collect and compare the prevalence of alcohol-induced pancreatitis and alcoholic gastritis in adults 18 years and over.
Cannabis Use and Alcohol-Induced Pancreatitis Alcohol-induced pancreatitis refers to progressive and sometimes irreversible damage of the pancreas gland caused by prolonged hazardous alcohol drinking.
In acute pancreatitis, inflammation of the pancreas lasts for a short period of time, causing mild to severe discomfort before resolving. Chronic pancreatitis is long-lasting inflammation of the pancreas. Both can be life threatening, and cause harm to other vital organs.
In the new study, researchers accessed discharge records data from 2012 to 2014 of the Nationwide Inpatient Sample. They identified three populations: those with gallstones, individuals with alcohol use disorder, and non-alcohol users with no gallstones from 2012-2014. The groups were compared with respect to cannabis use.
“Our findings suggest a reduced incidence of only alcohol-associated pancreatitis with cannabis use,” the researchers concluded.
The investigators found that cannabis use did not appear to have any impact on the risk of developing gallstone-related acute and chronic pancreatitis, prompting them to speculate that cannabis may be interacting with alcohol in the pancreas in unknown ways to prevent inflammation.
Previous studies have linked cannabis use to less severe acute alcohol-related pancreatitis symptoms.
Medical Cannabis Use and Alcoholic Gastritis Alcoholic gastritis is caused when excessive alcohol use irritates or even erodes parts of the stomach lining, leaving it exposed to digestive acids.
To compare the prevalence of alcoholic gastritis in heavy drinkers who use cannabis and those who do not, researchers accessed hospital discharge records of adults from 2014 of the National Inpatient Sample.
The researchers found that heavy drinkers who concurrently consumed cannabis had a 25 percent decreased probability of developing alcoholic gastritis compared to non-cannabis heavy drinkers.
“We reveal that risky alcohol drinking combined with cannabis use is associated with reduced prevalence of alcohol-associated gastritis in patients,” the study authors wrote.
“Given increased cannabis legislation globally, understanding if and how the specific ingredients in cannabis plant extract can be used in the treatment of alcoholic gastritis is paramount. In this regard, further molecular mechanistic studies are needed to delineate the mechanisms of our novel findings not only for alcoholic gastritis but also gastritis from other causes.”
Full text of the new study, “Reduced prevalence of alcoholic gastritis in hospitalized individuals who consume cannabis,” is available to purchase through Wiley Online Library. [https://onlinelibrary.wiley.com/doi/abs/10.1111/acer.13930]
6. Cannabidiol Treatment Might Promote Resilience to Cocaine and Methamphetamine Use Disorders: A Review of Possible Mechanisms
Among the past research the authors reviewed, studies have found:
Mice that were given CBD prior to consuming cocaine seemed to be better protected against acute liver inflammation and damage, as well as cocaine-induced seizures.
Mice that received high doses of CBD were less motivated to continue self-administering cocaine and meth in order to maintain their pleasurable effects.
When given CBD transdermally and over an extended period of time (versus a lower dose during a short-term treatment), rodents were less likely to relapse after being sober for 14 days.
People who were addicted to crack cocaine used marijuana to help them deal with withdrawal symptoms such as craving, impulsivity and paranoia, while another observational study found no difference in craving among cocaine-dependent people who consumed cannabis and those who did not.
Abstract: Currently, there are no approved pharmacotherapies for addiction to cocaine and other psychostimulant drugs. Several studies have proposed that cannabidiol (CBD) could be a promising treatment for substance use disorders. In the present work, the authors describe the scarce preclinical and human research about the actions of CBD on the effects of stimulant drugs, mainly cocaine and methamphetamine (METH). Additionally, the possible mechanisms underlying the therapeutic potential of CBD on stimulant use disorders are reviewed. CBD has reversed toxicity and seizures induced by cocaine, behavioural sensitization induced by amphetamines, motivation to self-administer cocaine and METH, context- and stress-induced reinstatement of cocaine and priming-induced reinstatement of METH seeking behaviours. CBD also potentiated the extinction of cocaine- and amphetamine-induced conditioned place preference (CPP), impaired the reconsolidation of cocaine CPP and prevented priming-induced reinstatement of METH CPP. Observational studies suggest that CBD may reduce problems related with crack-cocaine addiction, such as withdrawal symptoms, craving, impulsivity and paranoia (Fischer et al., 2015). The potential mechanisms involved in the protective effects of CBD on addiction to psychostimulant drugs include the prevention of drug-induced neuroadaptations (neurotransmitter and intracellular signalling pathways changes), the erasure of aberrant drug-memories, the reversion of cognitive deficits induced by psychostimulant drugs and the alleviation of mental disorders comorbid with psychostimulant abuse. Further, preclinical studies and future clinical trials are necessary to fully evaluate the potential of CBD as an intervention for cocaine and methamphetamine addictive disorders. [https://www.mdpi.com/1420-3049/24/14/2583/htm]