

Jason Barker
Albuquerque, NM 87109
SafeAccessNewMexico@gmail.com
Monday, November 11th 2019
Albuquerque, NM 87109
SafeAccessNewMexico@gmail.com
Monday, November 11th 2019
(Petitions provided to NMDOH
Medical Cannabis Program Office
on November 12th 2019
via hand delivery)
New Mexico State Department of Health
Medical Cannabis Advisory Board
Medical Cannabis Program
PO Box 26110
Santa Fe, NM, 87502-6110
All Petitions Can Be Viewed Online At: LECUA NM MCP MCAB Petitions (http://lecuanmmcpmcabpetitions.blogspot.com/)
Table of Contents
Pg. 1 Cover Page
Pg. 2 Petition Introduction
Pg. 3 Petition Purpose and Background
Pg. 5-16 ADD/ADHD and TS
Pg. 16-28 Anxiety Disorder
Pg. 28-31 Tourette’s
Pg. 31 Relief Requested In Petition
Pg.32-33 References
Pg.33-40 New Research since Petitioned Health Conditions were last approved in 2017
New Mexico’s medical cannabis history started in 1978, after public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis. The New Mexico’s medical cannabis program (MCP) is the only program in the U.S. that places sole responsibility for regulation on the state’s Department of Health. Doctors must comply with state requirements for patients to be considered for applying to the medical cannabis program.
We have a sound law in the Lynn and Erin Compassionate Use Act, as Section 2 reads; PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
Mosby’s Medical Dictionary states that “medical treatment” means; the management and care of a patient to combat disease or disorder. Medical treatment includes: Using prescription medications, or use of a non-prescription drug at prescription strength; and or treatment of disease by hygienic and pharmacologic remedies, as distinguished from invasive surgical procedures. Treatment may be pharmacologic, using drugs; surgical, involving operative procedures; or supportive, building the patient's strength. It may be specific for the disorder, or symptomatic to relieve symptoms without effecting a cure.(Mosby's Medical Dictionary, 9th edition.)
What is a chronic medical condition?
A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear. Harvard Medical Dictionary defines chronic as: Any condition that lasts a long time or recurs over time; chronic pain as: Pain that persists after an injury has healed or a disease is over; and chronic pain syndrome as : Long-term, severe pain that doesn't spring from an injury or illness, that interferes with daily life, and is often accompanied by other problems, such as depression, irritability, and anxiety.
What is the meaning of debilitating?
Something that's debilitating seriously affects someone or something's strength or ability to carry on with regular activities, like a debilitating illness. Debilitating comes from the Latin word debilis, meaning "weak." That's why you'll often see the adjective used to describe illness, despite the negative reference.
Petition Purpose and Background:
This Petition: Requesting The Inclusion Of A New Medical Condition(s): ADD/ADHD Anxiety, And Tourette's Syndrome is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
Who Should Qualify for Medical Cannabis Use?
According to Americans For Safe Access Policy Studies & Research:
Background: The most fundamental aspect of medical cannabis laws is the relationship between a patient and their physician. It is often only the physician and the patient that possess information about a patient’s health condition. However, many public officials and others who oppose medical cannabis laws often make assumptions about people’s health. The media have even fomented such inappropriate assumptions by naming a category of patients “Young Able Bodied Males,” condemning certain patients by visual assessment alone.
Findings: The health care information discussed between a patient and physician is considered private and protected under federal HIPAA laws. It is typically the purview of state medical boards to assess whether a physician has inappropriately recommended cannabis to someone who should not be qualified. Studies have shown in some medical cannabis states that the majority of patients suffer from chronic pain, an ailment that is not obviously detectable by another person. Nevertheless, police will often harass and arrest patients based on the assumption that someone is faking their illness.
Position: Medical professionals should have an unrestricted ability to recommend cannabis therapeutics and that should not be impacted by law enforcement’s perceptions.
Americans For Safe Access policy further states:
“Qualifying medical condition” shall mean any condition for which treatment with medical cannabis would be beneficial, as determined by a patient's qualified medical professional, including but not limited to cancer, glaucoma, positive status for human immunodeficiency virus, acquired immune deficiency syndrome (AIDS), hepatitis C, amyotrophic lateral sclerosis (ALS), Crohn’s disease, Parkinson’s disease, post-traumatic stress disorder, arthritis, chronic pain, neuropathic and other intractable chronic pain, and multiple sclerosis.
“Qualifying patient” shall mean a person who has a written recommendation from a qualified medical professional for the medical use of cannabis.
ADD/ADHD Anxiety, And Tourette's Syndrome
Adults with ADHD are likely to have an anxiety disorder, depression, bipolar disorder, or other comorbid psychiatric disorder. (The term “comorbid” refers to a condition that exists with another.) About 50 percent of adults with ADHD also suffer from an anxiety disorder.
[https://adaa.org/understanding-anxiety/related-illnesses/other-related-conditions/adult-adhd]
Tic Disorders and Tourette SyndromeFrom the Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD)
[http://www.chadd.org/]
The Diagnostic and Statistical Manual, Fifth Edition (DSM 5), outlines the symptoms of three tic disorders: provisional tic disorder, persistent (chronic) motor or vocal tic disorder, and Tourette’s disorder. Each of these disorders is characterized by the presence of motor or vocal tics, and which disorder is diagnosed is determined by the severity of the symptoms. The most severe of these is Tourette’s disorder or Tourette’s Syndrome.
Tourette Syndrome is a complex, genetically inherited disorder whose primary symptoms include tics (both motor and vocal) lasting for more than one year, beginning before age 18. Tourette Syndrome is usually mild, and a large number of patients tend to improve as they get older. Tourette Syndrome is often accompanied by other conditions including ADHD and obsessive-compulsive disorder in more than half of the patients as well as learning disabilities and mood disorders. More than half (57.1 percent) of patients with Tourette Syndrome have a family history of the disorder.
Tics or Tourette Syndrome
ADHD frequently co-occurs in children with Tourette Syndrome. Less than 10 percent of those with ADHD have Tourette’s, but 60 to 80 percent of children with Tourette Syndrome have ADHD. The ADHD diagnosis usually precedes the onset of the motor or vocal tics of Tourette’s, although sometimes the two occur together. Some children with ADHD may develop a simple motor tic disorder that first appears during the course of their treatment for ADHD. While these two conditions appear linked in time, most experts believe that the co-occurrence in most cases is purely coincidental and not caused by ADHD or its treatment.
ADD/ADHDADD is considered an outdated term for ADHD. Attention deficit hyperactivity disorder (ADHD) is one of the most common childhood disorders. ADHD is a broad term, and the condition can vary from person to person. There are an estimated 6.4 million diagnosed children in the United States, according to the Centers for Disease Control and Prevention.
This condition is sometimes called attention deficit disorder (ADD), but this is an outdated term. The term was once used to refer to someone who had trouble focusing but was not hyperactive. The American Psychiatric Association released the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) in May 2013. The DSM-5 changed the criteria to diagnose someone with ADHD.
1. Inattentive - Inattentive ADHD is what’s usually meant when someone uses the term ADD. This means a person shows enough symptoms of inattention (or easy distractibility) but isn’t hyperactive or impulsive.
2. Hyperactive/impulsive - This type occurs when a person has symptoms of hyperactivity and impulsivity but not inattention.
3. Combined - Combined ADHD is when a person has symptoms of inattention, hyperactivity, and impulsivity.
Inattention, hyperactivity, and impulsivity are important symptoms for an ADHD diagnosis. In addition, a child or adult must meet the following criteria to be diagnosed with ADHD:
Adults with ADHD have typically had the disorder since childhood, but it may not be diagnosed until later in life. An evaluation usually occurs at the prompting of a peer, family member, or co-worker who observes problems at work or in relationships.
Adults can have any of the three subtypes of ADHD. Adult ADHD symptoms can differ from those of children because of the relative maturity of adults, as well as physical differences between adults and children.
The symptoms of ADHD can range from mild to severe, depending on a person’s unique physiology and environment. Some people are mildly inattentive or hyperactive when they perform a task they don’t enjoy, but they have the ability to focus on tasks they like. Others may experience more severe symptoms. These can affect school, work, and social situations.
Symptoms are often more severe in unstructured group situations than in structured situations with rewards. For example, a playground is a more unstructured group situation. A classroom may represent a structured and rewards-based environment.
Other conditions, such as depression, anxiety, or a learning disability may worsen symptoms.
Some people report that symptoms go away with age. An adult with ADHD who was hyperactive as a child may find that they’re now able to remain seated or curb some impulsivity.
What is a tic?
Tics are defined as sudden, rapid, non-rhythmic movements or sounds that people do repeatedly. They may commonly include such behaviors as eye blinking, mouth opening, sniffing or throat clearing. Tics are common in childhood but do not continue into adulthood in most cases. Males are more affected than females in a ratio of 4.4 to 1. The occurrence of tics can be temporary, lasting less than 12 months, or chronic.
Tics can be either simple or complex. Simple tics are short in duration and involve a single muscle group. Complex tics are longer in duration and often include a series of simple tics. Motor tics may range from simple movements such as eye blinking, lip licking, or mouth opening to more complex movements like facial grimacing, head movements, shoulder shrugging or combinations of these. Vocal tics many include throat clearing; coughing; barking; unnecessary belching; or more complex vocalizations such as repeating parts of words or phrases or, in rare cases, saying obscene words.
Medication Currently UsedIf you’re taking medicine for ADHD or Tourette’s, what you’re taking likely is a controlled substance. That means that the federal government regulates how the drug is made, prescribed, and dispensed.
The majority of ADHD stimulant medications, such as dextroamphetamine-amphetamine (Adderall, Adderall XR), lisdexamfetamine (Vyvanse), and methylphenidate (Ritalin), fall into the Schedule II category. They're legal, but they’re considered dangerous because of their high risk of abuse and dependence. Other Schedule II drugs include painkillers like OxyContin and Vicodin.
After a proper assessment and trying behavior therapy, medication may still be necessary in children with ADHD and Tourette Syndrome. Mild symptoms can usually be treated with clonidine or guanfacine. Clonidine can be given by skin patch or in pill form. Clonidine or guanfacine have the advantage of treating all the symptoms of TS―the tics, the ADHD, obsessive-compulsive behaviors, and oppositional and other behaviors. The major side effect of these two medications is falling asleep or tiredness if the dose is too high or raised too rapidly.
Any treatment with stimulant medications should be closely monitored for side effects, especially the presence or increase of tics. In the past, the use of stimulants had not been recommended when tics or Tourette Syndrome was present; however, recent studies report that short-term use of stimulant medications, especially methylphenidate (Ritalin, Concerta), seem to be safe and well tolerated in children with chronic tics or Tourette Syndrome with co-occurring ADHD. Children who were given methylphenidate did not develop more frequent tics when compared with those who were not given the medication. However, frequency of tics seems to be higher with dextroamphetamines (Dexedrine, ProCentra) than compared with methylphenidate.
If a child has already been diagnosed and treated with stimulants and significant tics develop, the physician may elect to stop treatment with stimulants, decrease the dose or change to other stimulant medication until the tics are treated and under control. In some cases, the benefits of the stimulant medication outweigh the mild impact of the tics. Other medications may also benefit the ADHD symptoms and have some impact over the tics.
Hallucinations such as seeing snakes, insects, or worms that aren't there are another rare side effect of some ADHD medications. And some kids have dramatic behavior changes, ranging from extremely angry, aggressive, anxious, or manic to emotionally flat and unresponsive.
Stimulant medications on the market today, such as Adderall, Ritalin, Concerta, Metadate, Vyvanse, Focalin, Daytrana, are all variations on just two molecules, amphetamine and methylphenidate. Both amphetamine and methylphenidate mimic the action of dopamine in the brain. Many scholarly studies - some of which are listed below - have now demonstrated that methylphenidate and amphetamine can cause lasting changes to those areas of the developing brain where dopamine receptors are found. The disrupting effects appear to be centered on the nucleus accumbens. This is not surprising, because the nucleus accumbens has a high density of dopamine receptors.
William Carlezon at Harvard was one of the early leading investigators in this field. You might begin by reading three of his papers on this topic:
• Carlezon, Mague, and Andersen, “Enduring behavioral effects of early exposure to methylphenidate in rats,” Biological Psychiatry, 2003, 54:1330-1337.
• Carlezon and Konradi, “Understanding the neurobiological consequences of early exposure to psychotropic drugs,” Neuropharmacology, 2004, 47 Suppl 1:47-60
• Mague, Andersen, and Carlezon, “Early developmental exposure to methylphenidate reduces cocaine-induced potentiation of brain stimulation reward in rats,” Biological Psychiatry, 2005, 57:120-125.
More recently, Dr. Carlezon has written a recent review emphasizing the role of the nucleus accumbens in motivation: see his paper, “Biological substrates of reward and aversion: a nucleus accumbens activity hypothesis,” Neuropharmacology, 2009, 56 Supp 1:122-132.
Terry Robinson and Bryan Kolb at the University of Michigan were among the first to demonstrate that low-dose amphetamine leads to damage to dendrites and dendritic spines in the nucleus accumbens. They reviewed this emerging field in their article "Structural plasticity associated with exposure to drugs of abuse,” Neuropharmacology, 2004, 47:33-46. They first documented this finding in their 1997 paper, “Persistent structural modifications in nucleus accumbens and prefrontal cortex neurons produced by previous experiences with amphetamine,” Journal of Neuroscience, 17:8491-8497.
Other relevant articles include:
• S. P. Onn and A. A. Grace, “Amphetamine Withdrawal Alters Bistable States and Cellular Coupling in Rat Prefrontal Cortex and Nucleus Accumbens Neurons Recorded in Vivo”, Journal of Neuroscience, volume 20, pp. 2332–2345, 2000.
• Y. Li and J. A. Kauer, “Repeated Exposure to Amphetamine Disrupts Dopaminergic Modulation of Excitatory Synaptic Plasticity and Neurotransmission in Nucleus Accumbens,” Synapse, volume 51, pp. 1–10, 2004.
• R. Diaz-Heijtz, B. Kolb, and H. Forssberg, “Can a Therapeutic Dose of Amphetamine During Pre-adolescence Modify the Pattern of Synaptic Organization in the Brain?” European Journal of Neuroscience, volume 18, pp. 3394–3399, 2003.
• Louk J. Vanderschuren, E. Donné Schmidt, T. J. De Vries, et al., “ A Single Exposure to Amphetamine is Sufficient to Induce Long-term Behavioral, Neuroendocrine, and Neurochemical Sensitization in Rats,” Journal of Neuroscience, volume 19, pp. 9579–9586, 1999.
Those are some of the “classic” studies on this topic. For more recent updates, you might begin by reading:
· Russo et al., 2010: “The addicted synapse: mechanisms of synaptic and structural plasticity in the nucleus accumbens,” Trends in Neuroscience, 33:267 – 276.
· Mameli & Lüscher, 2011: “Synaptic plasticity and addiction: learning mechanisms gone awry,” Neuropharmacology, 61:1052-1059.
· Margery Pardey et al., 2012 “Long-term effects of chronic oral Ritalin administration on cognitive and neural development in adolescent Wistar Kyoto Rats”, Brain Sciences, 2:375-404.
· Esther Gramage et al., 2013, “Periadolescent amphetamine treatment causes transient cognitive disruptions and long-term changes in hippocampal LTP”, Addiction Biology, 18:19-29.
Studies like these strongly suggest that even short-term, low-dose exposure to amphetamine or to methylphenidate, particularly in the juvenile brain, may induce long-lasting changes both neurally (particularly in the nucleus accumbens and hippocampus) and behaviorally. In some studies, e.g. a 2010 report from Canada, the effects are dramatic in the juvenile or adolescent, but absent in the adult brain. Remember that in humans, longitudinal studies suggest that females do not reach full maturity in terms of brain development until about 20 to 22 years of age; males do not reach full maturity in terms of brain development until 28 to 30 years of age.(3)
Case Report - Cannabis improves symptoms of ADHDBy Peter Strohbeck-Kuehner, Gisela Skopp, Rainer Mattern
Institute of Legal- and Traffic Medicine, Heidelberg University Medical Centre, Voss Str. 2, D-69115 Heidelberg, Germany
Abstract
Attention-deficit/hyperactivity disorder (ADHD) is characterized by attention deficits and an altered activation level. The purpose of this case investigation was to highlight that people with ADHD can benefit in some cases from the consumption of THC. A 28-year old male, who showed improper behaviour and appeared to be very maladjusted and inattentive while sober, appeared to be completely inconspicuous while having a very high blood plasma level of delta-9- tetrahydrocannabinol (THC). Performance tests, which were conducted with the test batteries ART2020 and TAP provided sufficient and partly over-averaged results in driving related performance.
Thus, it has to be considered, that in the case of ADHD, THC can have atypical effects
and can even lead to an enhanced driving related performance.
Keywords: ADHD, cannabis, performance, driving
This article can be downloaded, printed and distributed freely for any non-commercial purposes, provided the original work is properly cited (see copyright info below). Available online at www.cannabis-med.org (http://cannabis-med.org/data/pdf/en_2008_01_1.pdf)
Author's address: Peter Strohbeck-Kuehner, peter.strohbeck@med.uni-heidelberg.de
New Mexico State Department of Health
Medical Cannabis Advisory Board
Medical Cannabis Program
PO Box 26110
Santa Fe, NM, 87502-6110
Petition: Requesting The Inclusion Of A New Medical Condition(s): ADD/ADHD, Anxiety Disorder, And Tourette's Syndrome
All Petitions Can Be Viewed Online At: LECUA NM MCP MCAB Petitions (http://lecuanmmcpmcabpetitions.blogspot.com/)
Table of Contents
Pg. 1 Cover Page
Pg. 2 Petition Introduction
Pg. 3 Petition Purpose and Background
Pg. 5-16 ADD/ADHD and TS
Pg. 16-28 Anxiety Disorder
Pg. 28-31 Tourette’s
Pg. 31 Relief Requested In Petition
Pg.32-33 References
Pg.33-40 New Research since Petitioned Health Conditions were last approved in 2017
Petition: Requesting The Inclusion Of A New Medical Condition(s): ADD/ADHD And Tourette's Syndrome
New Mexico’s medical cannabis history started in 1978, after public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis. The New Mexico’s medical cannabis program (MCP) is the only program in the U.S. that places sole responsibility for regulation on the state’s Department of Health. Doctors must comply with state requirements for patients to be considered for applying to the medical cannabis program.
We have a sound law in the Lynn and Erin Compassionate Use Act, as Section 2 reads; PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
“ARTICLE 2B. LYNN AND ERIN COMPASSIONATE USE ACT N.M. Stat. Ann. § 26-2B-2 (2009) § 26-2B-2. Purpose of act
The purpose of the Lynn and Erin Compassionate Use Act [26-2B-1 NMSA 1978] is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments. HISTORY: Laws 2007, ch. 210, § 2. EFFECTIVE DATES. --Laws 2007, ch. 210, § 12 makes the act effective July 1, 2007.”
Mosby’s Medical Dictionary states that “medical treatment” means; the management and care of a patient to combat disease or disorder. Medical treatment includes: Using prescription medications, or use of a non-prescription drug at prescription strength; and or treatment of disease by hygienic and pharmacologic remedies, as distinguished from invasive surgical procedures. Treatment may be pharmacologic, using drugs; surgical, involving operative procedures; or supportive, building the patient's strength. It may be specific for the disorder, or symptomatic to relieve symptoms without effecting a cure.(Mosby's Medical Dictionary, 9th edition.)
What is a chronic medical condition?
A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear. Harvard Medical Dictionary defines chronic as: Any condition that lasts a long time or recurs over time; chronic pain as: Pain that persists after an injury has healed or a disease is over; and chronic pain syndrome as : Long-term, severe pain that doesn't spring from an injury or illness, that interferes with daily life, and is often accompanied by other problems, such as depression, irritability, and anxiety.
What is the meaning of debilitating?
Something that's debilitating seriously affects someone or something's strength or ability to carry on with regular activities, like a debilitating illness. Debilitating comes from the Latin word debilis, meaning "weak." That's why you'll often see the adjective used to describe illness, despite the negative reference.
Petition Purpose and Background:
The purpose of this Petition: Requesting The Inclusion Of A New Medical Condition(s): ADD/ADHD, Anxiety And Tourette's Syndrome
This Petition: Requesting The Inclusion Of A New Medical Condition(s): ADD/ADHD Anxiety, And Tourette's Syndrome is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
Who Should Qualify for Medical Cannabis Use?
According to Americans For Safe Access Policy Studies & Research:
Background: The most fundamental aspect of medical cannabis laws is the relationship between a patient and their physician. It is often only the physician and the patient that possess information about a patient’s health condition. However, many public officials and others who oppose medical cannabis laws often make assumptions about people’s health. The media have even fomented such inappropriate assumptions by naming a category of patients “Young Able Bodied Males,” condemning certain patients by visual assessment alone.
Findings: The health care information discussed between a patient and physician is considered private and protected under federal HIPAA laws. It is typically the purview of state medical boards to assess whether a physician has inappropriately recommended cannabis to someone who should not be qualified. Studies have shown in some medical cannabis states that the majority of patients suffer from chronic pain, an ailment that is not obviously detectable by another person. Nevertheless, police will often harass and arrest patients based on the assumption that someone is faking their illness.
Position: Medical professionals should have an unrestricted ability to recommend cannabis therapeutics and that should not be impacted by law enforcement’s perceptions.
Americans For Safe Access policy further states:
“Qualifying medical condition” shall mean any condition for which treatment with medical cannabis would be beneficial, as determined by a patient's qualified medical professional, including but not limited to cancer, glaucoma, positive status for human immunodeficiency virus, acquired immune deficiency syndrome (AIDS), hepatitis C, amyotrophic lateral sclerosis (ALS), Crohn’s disease, Parkinson’s disease, post-traumatic stress disorder, arthritis, chronic pain, neuropathic and other intractable chronic pain, and multiple sclerosis.
“Qualifying patient” shall mean a person who has a written recommendation from a qualified medical professional for the medical use of cannabis.
ADD/ADHD Anxiety, And Tourette's Syndrome
Adults with ADHD are likely to have an anxiety disorder, depression, bipolar disorder, or other comorbid psychiatric disorder. (The term “comorbid” refers to a condition that exists with another.) About 50 percent of adults with ADHD also suffer from an anxiety disorder.
[https://adaa.org/understanding-anxiety/related-illnesses/other-related-conditions/adult-adhd]
Tic Disorders and Tourette SyndromeFrom the Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD)
[http://www.chadd.org/]
The Diagnostic and Statistical Manual, Fifth Edition (DSM 5), outlines the symptoms of three tic disorders: provisional tic disorder, persistent (chronic) motor or vocal tic disorder, and Tourette’s disorder. Each of these disorders is characterized by the presence of motor or vocal tics, and which disorder is diagnosed is determined by the severity of the symptoms. The most severe of these is Tourette’s disorder or Tourette’s Syndrome.
Tourette Syndrome is a complex, genetically inherited disorder whose primary symptoms include tics (both motor and vocal) lasting for more than one year, beginning before age 18. Tourette Syndrome is usually mild, and a large number of patients tend to improve as they get older. Tourette Syndrome is often accompanied by other conditions including ADHD and obsessive-compulsive disorder in more than half of the patients as well as learning disabilities and mood disorders. More than half (57.1 percent) of patients with Tourette Syndrome have a family history of the disorder.
Tics or Tourette Syndrome
ADHD frequently co-occurs in children with Tourette Syndrome. Less than 10 percent of those with ADHD have Tourette’s, but 60 to 80 percent of children with Tourette Syndrome have ADHD. The ADHD diagnosis usually precedes the onset of the motor or vocal tics of Tourette’s, although sometimes the two occur together. Some children with ADHD may develop a simple motor tic disorder that first appears during the course of their treatment for ADHD. While these two conditions appear linked in time, most experts believe that the co-occurrence in most cases is purely coincidental and not caused by ADHD or its treatment.
ADD/ADHDADD is considered an outdated term for ADHD. Attention deficit hyperactivity disorder (ADHD) is one of the most common childhood disorders. ADHD is a broad term, and the condition can vary from person to person. There are an estimated 6.4 million diagnosed children in the United States, according to the Centers for Disease Control and Prevention.
This condition is sometimes called attention deficit disorder (ADD), but this is an outdated term. The term was once used to refer to someone who had trouble focusing but was not hyperactive. The American Psychiatric Association released the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) in May 2013. The DSM-5 changed the criteria to diagnose someone with ADHD.
1. Inattentive - Inattentive ADHD is what’s usually meant when someone uses the term ADD. This means a person shows enough symptoms of inattention (or easy distractibility) but isn’t hyperactive or impulsive.
2. Hyperactive/impulsive - This type occurs when a person has symptoms of hyperactivity and impulsivity but not inattention.
3. Combined - Combined ADHD is when a person has symptoms of inattention, hyperactivity, and impulsivity.
Inattention, hyperactivity, and impulsivity are important symptoms for an ADHD diagnosis. In addition, a child or adult must meet the following criteria to be diagnosed with ADHD:
- displays several symptoms before the age of 12
- has symptoms in more than one setting, such as school, at home, with friends, or during other activities
- shows clear evidence that the symptoms interfere with their functioning at school, work, or in social situations
- has symptoms that are not explained by another condition, such as mood or anxiety disorders
Adults with ADHD have typically had the disorder since childhood, but it may not be diagnosed until later in life. An evaluation usually occurs at the prompting of a peer, family member, or co-worker who observes problems at work or in relationships.
Adults can have any of the three subtypes of ADHD. Adult ADHD symptoms can differ from those of children because of the relative maturity of adults, as well as physical differences between adults and children.
The symptoms of ADHD can range from mild to severe, depending on a person’s unique physiology and environment. Some people are mildly inattentive or hyperactive when they perform a task they don’t enjoy, but they have the ability to focus on tasks they like. Others may experience more severe symptoms. These can affect school, work, and social situations.
Symptoms are often more severe in unstructured group situations than in structured situations with rewards. For example, a playground is a more unstructured group situation. A classroom may represent a structured and rewards-based environment.
Other conditions, such as depression, anxiety, or a learning disability may worsen symptoms.
Some people report that symptoms go away with age. An adult with ADHD who was hyperactive as a child may find that they’re now able to remain seated or curb some impulsivity.
What is a tic?
Tics are defined as sudden, rapid, non-rhythmic movements or sounds that people do repeatedly. They may commonly include such behaviors as eye blinking, mouth opening, sniffing or throat clearing. Tics are common in childhood but do not continue into adulthood in most cases. Males are more affected than females in a ratio of 4.4 to 1. The occurrence of tics can be temporary, lasting less than 12 months, or chronic.
Tics can be either simple or complex. Simple tics are short in duration and involve a single muscle group. Complex tics are longer in duration and often include a series of simple tics. Motor tics may range from simple movements such as eye blinking, lip licking, or mouth opening to more complex movements like facial grimacing, head movements, shoulder shrugging or combinations of these. Vocal tics many include throat clearing; coughing; barking; unnecessary belching; or more complex vocalizations such as repeating parts of words or phrases or, in rare cases, saying obscene words.
Medication Currently UsedIf you’re taking medicine for ADHD or Tourette’s, what you’re taking likely is a controlled substance. That means that the federal government regulates how the drug is made, prescribed, and dispensed.
The majority of ADHD stimulant medications, such as dextroamphetamine-amphetamine (Adderall, Adderall XR), lisdexamfetamine (Vyvanse), and methylphenidate (Ritalin), fall into the Schedule II category. They're legal, but they’re considered dangerous because of their high risk of abuse and dependence. Other Schedule II drugs include painkillers like OxyContin and Vicodin.
After a proper assessment and trying behavior therapy, medication may still be necessary in children with ADHD and Tourette Syndrome. Mild symptoms can usually be treated with clonidine or guanfacine. Clonidine can be given by skin patch or in pill form. Clonidine or guanfacine have the advantage of treating all the symptoms of TS―the tics, the ADHD, obsessive-compulsive behaviors, and oppositional and other behaviors. The major side effect of these two medications is falling asleep or tiredness if the dose is too high or raised too rapidly.
Any treatment with stimulant medications should be closely monitored for side effects, especially the presence or increase of tics. In the past, the use of stimulants had not been recommended when tics or Tourette Syndrome was present; however, recent studies report that short-term use of stimulant medications, especially methylphenidate (Ritalin, Concerta), seem to be safe and well tolerated in children with chronic tics or Tourette Syndrome with co-occurring ADHD. Children who were given methylphenidate did not develop more frequent tics when compared with those who were not given the medication. However, frequency of tics seems to be higher with dextroamphetamines (Dexedrine, ProCentra) than compared with methylphenidate.
If a child has already been diagnosed and treated with stimulants and significant tics develop, the physician may elect to stop treatment with stimulants, decrease the dose or change to other stimulant medication until the tics are treated and under control. In some cases, the benefits of the stimulant medication outweigh the mild impact of the tics. Other medications may also benefit the ADHD symptoms and have some impact over the tics.
Hallucinations such as seeing snakes, insects, or worms that aren't there are another rare side effect of some ADHD medications. And some kids have dramatic behavior changes, ranging from extremely angry, aggressive, anxious, or manic to emotionally flat and unresponsive.
Stimulant medications on the market today, such as Adderall, Ritalin, Concerta, Metadate, Vyvanse, Focalin, Daytrana, are all variations on just two molecules, amphetamine and methylphenidate. Both amphetamine and methylphenidate mimic the action of dopamine in the brain. Many scholarly studies - some of which are listed below - have now demonstrated that methylphenidate and amphetamine can cause lasting changes to those areas of the developing brain where dopamine receptors are found. The disrupting effects appear to be centered on the nucleus accumbens. This is not surprising, because the nucleus accumbens has a high density of dopamine receptors.
William Carlezon at Harvard was one of the early leading investigators in this field. You might begin by reading three of his papers on this topic:
• Carlezon, Mague, and Andersen, “Enduring behavioral effects of early exposure to methylphenidate in rats,” Biological Psychiatry, 2003, 54:1330-1337.
• Carlezon and Konradi, “Understanding the neurobiological consequences of early exposure to psychotropic drugs,” Neuropharmacology, 2004, 47 Suppl 1:47-60
• Mague, Andersen, and Carlezon, “Early developmental exposure to methylphenidate reduces cocaine-induced potentiation of brain stimulation reward in rats,” Biological Psychiatry, 2005, 57:120-125.
More recently, Dr. Carlezon has written a recent review emphasizing the role of the nucleus accumbens in motivation: see his paper, “Biological substrates of reward and aversion: a nucleus accumbens activity hypothesis,” Neuropharmacology, 2009, 56 Supp 1:122-132.
Terry Robinson and Bryan Kolb at the University of Michigan were among the first to demonstrate that low-dose amphetamine leads to damage to dendrites and dendritic spines in the nucleus accumbens. They reviewed this emerging field in their article "Structural plasticity associated with exposure to drugs of abuse,” Neuropharmacology, 2004, 47:33-46. They first documented this finding in their 1997 paper, “Persistent structural modifications in nucleus accumbens and prefrontal cortex neurons produced by previous experiences with amphetamine,” Journal of Neuroscience, 17:8491-8497.
Other relevant articles include:
• S. P. Onn and A. A. Grace, “Amphetamine Withdrawal Alters Bistable States and Cellular Coupling in Rat Prefrontal Cortex and Nucleus Accumbens Neurons Recorded in Vivo”, Journal of Neuroscience, volume 20, pp. 2332–2345, 2000.
• Y. Li and J. A. Kauer, “Repeated Exposure to Amphetamine Disrupts Dopaminergic Modulation of Excitatory Synaptic Plasticity and Neurotransmission in Nucleus Accumbens,” Synapse, volume 51, pp. 1–10, 2004.
• R. Diaz-Heijtz, B. Kolb, and H. Forssberg, “Can a Therapeutic Dose of Amphetamine During Pre-adolescence Modify the Pattern of Synaptic Organization in the Brain?” European Journal of Neuroscience, volume 18, pp. 3394–3399, 2003.
• Louk J. Vanderschuren, E. Donné Schmidt, T. J. De Vries, et al., “ A Single Exposure to Amphetamine is Sufficient to Induce Long-term Behavioral, Neuroendocrine, and Neurochemical Sensitization in Rats,” Journal of Neuroscience, volume 19, pp. 9579–9586, 1999.
Those are some of the “classic” studies on this topic. For more recent updates, you might begin by reading:
· Russo et al., 2010: “The addicted synapse: mechanisms of synaptic and structural plasticity in the nucleus accumbens,” Trends in Neuroscience, 33:267 – 276.
· Mameli & Lüscher, 2011: “Synaptic plasticity and addiction: learning mechanisms gone awry,” Neuropharmacology, 61:1052-1059.
· Margery Pardey et al., 2012 “Long-term effects of chronic oral Ritalin administration on cognitive and neural development in adolescent Wistar Kyoto Rats”, Brain Sciences, 2:375-404.
· Esther Gramage et al., 2013, “Periadolescent amphetamine treatment causes transient cognitive disruptions and long-term changes in hippocampal LTP”, Addiction Biology, 18:19-29.
Studies like these strongly suggest that even short-term, low-dose exposure to amphetamine or to methylphenidate, particularly in the juvenile brain, may induce long-lasting changes both neurally (particularly in the nucleus accumbens and hippocampus) and behaviorally. In some studies, e.g. a 2010 report from Canada, the effects are dramatic in the juvenile or adolescent, but absent in the adult brain. Remember that in humans, longitudinal studies suggest that females do not reach full maturity in terms of brain development until about 20 to 22 years of age; males do not reach full maturity in terms of brain development until 28 to 30 years of age.(3)
Related Clinical Information to ADHD, Tourette Syndrome, and Medical Cannabis
Institute of Legal- and Traffic Medicine, Heidelberg University Medical Centre, Voss Str. 2, D-69115 Heidelberg, Germany
Abstract
Attention-deficit/hyperactivity disorder (ADHD) is characterized by attention deficits and an altered activation level. The purpose of this case investigation was to highlight that people with ADHD can benefit in some cases from the consumption of THC. A 28-year old male, who showed improper behaviour and appeared to be very maladjusted and inattentive while sober, appeared to be completely inconspicuous while having a very high blood plasma level of delta-9- tetrahydrocannabinol (THC). Performance tests, which were conducted with the test batteries ART2020 and TAP provided sufficient and partly over-averaged results in driving related performance.
Thus, it has to be considered, that in the case of ADHD, THC can have atypical effects
and can even lead to an enhanced driving related performance.
Keywords: ADHD, cannabis, performance, driving
This article can be downloaded, printed and distributed freely for any non-commercial purposes, provided the original work is properly cited (see copyright info below). Available online at www.cannabis-med.org (http://cannabis-med.org/data/pdf/en_2008_01_1.pdf)
Author's address: Peter Strohbeck-Kuehner, peter.strohbeck@med.uni-heidelberg.de
Subtypes of attention deficit-hyperactivity disorder (ADHD) and cannabis use.
Loflin M1, Earleywine M, De Leo J, Hobkirk A. - Author information
Abstract
The current study examined the association between subtypes of attention-deficit/hyperactivity disorder (ADHD) and cannabis use within a sample of 2811 current users. Data were collected in 2012 from a national U.S. survey of cannabis users. A series of logistic regression equations and chi-squares were assessed for proportional differences between users. When asked about the ADHD symptoms they have experienced when not using cannabis, a higher proportion of daily users met symptom criteria for an ADHD diagnoses of the subtypes that include hyperactive-impulsive symptoms than the inattentive subtype. For nondaily users, the proportions of users meeting symptom criteria did not differ by subtype. These results have implications for identifying which individuals with ADHD might be more likely to self-medicate using cannabis. Furthermore, these findings indirectly support research linking relevant cannabinoid receptors to regulatory control.
PMID:24093525 DOI: 10.3109/10826084.2013.841251 https://www.ncbi.nlm.nih.gov/pubmed/24093525
Impact of ADHD and cannabis use on executive functioning in young adults.
Tamm L1, Epstein JN, Lisdahl KM, Molina B, Tapert S, Hinshaw SP, Arnold LE, Velanova K, Abikoff H, Swanson JM; MTA Neuroimaging Group. Collaborators (28) Author information
Abstract
BACKGROUND:
Attention-deficit/hyperactivity disorder (ADHD) and cannabis use are each associated with specific cognitive deficits. Few studies have investigated the neurocognitive profile of individuals with both an ADHD history and regular cannabis use. The greatest cognitive impairment is expected among ADHD Cannabis Users compared to those with ADHD-only, Cannabis use-only, or neither.
METHODS:
Young adults (24.2 ± 1.2 years) with a childhood ADHD diagnosis who did (n=42) and did not (n=45) report past year ≥ monthly cannabis use were compared on neuropsychological measures to a local normative comparison group (LNCG) who did (n=20) and did not (n=21) report past year regular cannabis use. Age, gender, IQ, socioeconomic status, and past year alcohol and smoking were statistical covariates.
RESULTS:
The ADHD group performed worse than LNCG on verbal memory, processing speed, cognitive interference, decision-making, working memory, and response inhibition. No significant effects for cannabis use emerged. Interactions between ADHD and cannabis were non-significant. Exploratory analyses revealed that individuals who began using cannabis regularly before age 16 (n=27) may have poorer executive functioning (i.e., decision-making, working memory, and response inhibition), than users who began later (n=32); replication is warranted with a larger sample.
CONCLUSIONS:
A childhood diagnosis of ADHD, but not cannabis use in adulthood, was associated with executive dysfunction. Earlier initiation of cannabis use may be linked to poor cognitive outcomes and a significantly greater proportion of the ADHD group began using cannabis before age 16. Regular cannabis use starting after age 16 may not be sufficient to aggravate longstanding cognitive deficits characteristic of ADHD
[https://www.ncbi.nlm.nih.gov/pubmed/23992650]
Cannabinoids in attention-deficit/hyperactivity disorder: A randomised-controlled trial.
Cooper RE1, Williams E2, Seegobin S3, Tye C2, Kuntsi J2, Asherson P4. Author information
Abstract
Adults with ADHD describe self-medicating with cannabis, with some reporting a preference for cannabis over ADHD medications. A small number of psychiatrists in the US prescribe cannabis medication for ADHD, despite there being no evidence from randomised controlled studies. The EMA-C trial (Experimental Medicine in ADHD-Cannabinoids) was a pilot randomised placebo-controlled experimental study of a cannabinoid medication, Sativex Oromucosal Spray, in 30 adults with ADHD. The primary outcome was cognitive performance and activity level using the QbTest. Secondary outcomes included ADHD and emotional lability (EL) symptoms. From 17.07.14 to 18.06.15, 30 participants were randomly assigned to the active (n=15) or placebo (n=15) group. For the primary outcome, no significant difference was found in the ITT analysis although the overall pattern of scores was such that the active group usually had scores that were better than the placebo group (Est=-0.17, 95%CI-0.40 to 0.07, p=0.16, n=15/11 active/placebo).
Loflin M1, Earleywine M, De Leo J, Hobkirk A. - Author information
Abstract
The current study examined the association between subtypes of attention-deficit/hyperactivity disorder (ADHD) and cannabis use within a sample of 2811 current users. Data were collected in 2012 from a national U.S. survey of cannabis users. A series of logistic regression equations and chi-squares were assessed for proportional differences between users. When asked about the ADHD symptoms they have experienced when not using cannabis, a higher proportion of daily users met symptom criteria for an ADHD diagnoses of the subtypes that include hyperactive-impulsive symptoms than the inattentive subtype. For nondaily users, the proportions of users meeting symptom criteria did not differ by subtype. These results have implications for identifying which individuals with ADHD might be more likely to self-medicate using cannabis. Furthermore, these findings indirectly support research linking relevant cannabinoid receptors to regulatory control.
PMID:24093525 DOI: 10.3109/10826084.2013.841251 https://www.ncbi.nlm.nih.gov/pubmed/24093525
Impact of ADHD and cannabis use on executive functioning in young adults.
Tamm L1, Epstein JN, Lisdahl KM, Molina B, Tapert S, Hinshaw SP, Arnold LE, Velanova K, Abikoff H, Swanson JM; MTA Neuroimaging Group. Collaborators (28) Author information
Abstract
BACKGROUND:
Attention-deficit/hyperactivity disorder (ADHD) and cannabis use are each associated with specific cognitive deficits. Few studies have investigated the neurocognitive profile of individuals with both an ADHD history and regular cannabis use. The greatest cognitive impairment is expected among ADHD Cannabis Users compared to those with ADHD-only, Cannabis use-only, or neither.
METHODS:
Young adults (24.2 ± 1.2 years) with a childhood ADHD diagnosis who did (n=42) and did not (n=45) report past year ≥ monthly cannabis use were compared on neuropsychological measures to a local normative comparison group (LNCG) who did (n=20) and did not (n=21) report past year regular cannabis use. Age, gender, IQ, socioeconomic status, and past year alcohol and smoking were statistical covariates.
RESULTS:
The ADHD group performed worse than LNCG on verbal memory, processing speed, cognitive interference, decision-making, working memory, and response inhibition. No significant effects for cannabis use emerged. Interactions between ADHD and cannabis were non-significant. Exploratory analyses revealed that individuals who began using cannabis regularly before age 16 (n=27) may have poorer executive functioning (i.e., decision-making, working memory, and response inhibition), than users who began later (n=32); replication is warranted with a larger sample.
CONCLUSIONS:
A childhood diagnosis of ADHD, but not cannabis use in adulthood, was associated with executive dysfunction. Earlier initiation of cannabis use may be linked to poor cognitive outcomes and a significantly greater proportion of the ADHD group began using cannabis before age 16. Regular cannabis use starting after age 16 may not be sufficient to aggravate longstanding cognitive deficits characteristic of ADHD
[https://www.ncbi.nlm.nih.gov/pubmed/23992650]
Cannabinoids in attention-deficit/hyperactivity disorder: A randomised-controlled trial.
Cooper RE1, Williams E2, Seegobin S3, Tye C2, Kuntsi J2, Asherson P4. Author information
Abstract
Adults with ADHD describe self-medicating with cannabis, with some reporting a preference for cannabis over ADHD medications. A small number of psychiatrists in the US prescribe cannabis medication for ADHD, despite there being no evidence from randomised controlled studies. The EMA-C trial (Experimental Medicine in ADHD-Cannabinoids) was a pilot randomised placebo-controlled experimental study of a cannabinoid medication, Sativex Oromucosal Spray, in 30 adults with ADHD. The primary outcome was cognitive performance and activity level using the QbTest. Secondary outcomes included ADHD and emotional lability (EL) symptoms. From 17.07.14 to 18.06.15, 30 participants were randomly assigned to the active (n=15) or placebo (n=15) group. For the primary outcome, no significant difference was found in the ITT analysis although the overall pattern of scores was such that the active group usually had scores that were better than the placebo group (Est=-0.17, 95%CI-0.40 to 0.07, p=0.16, n=15/11 active/placebo).
For secondary outcomes Sativex was associated with a nominally significant improvement in hyperactivity/impulsivity (p=0.03) and a cognitive measure of inhibition (p=0.05), and a trend towards improvement for inattention (p=0.10) and EL (p=0.11). Per-protocol effects were higher. Results did not meet significance following adjustment for multiple testing. One serious (muscular seizures/spasms) and three mild adverse events occurred in the active group and one serious (cardiovascular problems) adverse event in the placebo group. Adults with ADHD may represent a subgroup of individuals who experience a reduction of symptoms and no cognitive impairments following cannabinoid use. While not definitive, this study provides preliminary evidence supporting the self-medication theory of cannabis use in ADHD and the need for further studies of the endocannabinoid system in ADHD. Copyright © 2017 Elsevier B.V. and ECNP. All rights reserved. KEYWORDS: Attention deficit-hyperactivity disorder; Cannabinoids; Randomised-controlled trial; Self-medication PMID: 28576350 DOI: 10.1016/j.euroneuro.2017.05.005 https://www.ncbi.nlm.nih.gov/pubmed/28576350
Delta 9-tetrahydrocannabinol (THC) is effective in the treatment of tics in Tourette syndrome: a 6-week randomized trial.
Delta 9-tetrahydrocannabinol (THC) is effective in the treatment of tics in Tourette syndrome: a 6-week randomized trial.
Müller-Vahl KR1, Schneider U, Prevedel H, Theloe K, Kolbe H, Daldrup T, Emrich HM. Author information
Abstract
BACKGROUND: Preliminary studies suggested that delta-9-tetrahydrocannabinol (THC), the major psychoactive ingredient of Cannabis sativa L., might be effective in the treatment of Tourette syndrome (TS). This study was performed to investigate for the first time under controlled conditions, over a longer-term treatment period, whether THC is effective and safe in reducing tics in TS.
METHOD: In this randomized, double-blind, placebo-controlled study, 24 patients with TS, according to DSM-III-R criteria, were treated over a 6-week period with up to 10 mg/day of THC. Tics were rated at 6 visits (visit 1, baseline; visits 2-4, during treatment period; visits 5-6, after withdrawal of medication) using the Tourette Syndrome Clinical Global Impressions scale (TS-CGI), the Shapiro Tourette-Syndrome Severity Scale (STSSS), the Yale Global Tic Severity Scale (YGTSS), the self-rated Tourette Syndrome Symptom List (TSSL), and a videotape-based rating scale.
RESULTS: Seven patients dropped out of the study or had to be excluded, but only 1 due to side effects. Using the TS-CGI, STSSS, YGTSS, and video rating scale, we found a significant difference (p <.05) or a trend toward a significant difference (p <.10) between THC and placebo groups at visits 2, 3, and/or 4. Using the TSSL at 10 treatment days (between days 16 and 41) there was a significant difference (p <.05) between both groups. ANOVA as well demonstrated a significant difference (p =.037). No serious adverse effects occurred.
CONCLUSION: Our results provide more evidence that THC is effective and safe in the treatment of tics. It, therefore, can be hypothesized that the central cannabinoid receptor system might play a role in TS pathology. (https://www.ncbi.nlm.nih.gov/pubmed/12716250)
Cannabinoids: possible role in pathophysiology and therapy of Gilles de la Tourette syndrome.
Müller-Vahl KR1, Kolbe H, Schneider U, Emrich HM. Author information
Abstract
High densities of cannabinoid receptors were found in the basal ganglia and hippocampus, indicating a putative functional role of cannabinoids in movement and behaviour. Anecdotal reports suggested beneficial effects of marijuana in Tourette's syndrome (TS). We therefore interviewed 64 TS patients with regard to use of marijuana and its influence on TS symptomatology. Of 17 patients (27%) who reported prior use of marijuana, 14 subjects (82%) experienced a reduction or complete remission of motor and vocal tics and an amelioration of premonitory urges and obsessive-compulsive symptoms. Our results provide more evidence that marijuana improves tics and behavioural disorders in TS. It can be speculated that cannabinoids might act through specific receptors, and that the cannabinoid system might play a major role in TS pathology. (https://www.ncbi.nlm.nih.gov/pubmed/9879795)
Abstract
BACKGROUND: Preliminary studies suggested that delta-9-tetrahydrocannabinol (THC), the major psychoactive ingredient of Cannabis sativa L., might be effective in the treatment of Tourette syndrome (TS). This study was performed to investigate for the first time under controlled conditions, over a longer-term treatment period, whether THC is effective and safe in reducing tics in TS.
METHOD: In this randomized, double-blind, placebo-controlled study, 24 patients with TS, according to DSM-III-R criteria, were treated over a 6-week period with up to 10 mg/day of THC. Tics were rated at 6 visits (visit 1, baseline; visits 2-4, during treatment period; visits 5-6, after withdrawal of medication) using the Tourette Syndrome Clinical Global Impressions scale (TS-CGI), the Shapiro Tourette-Syndrome Severity Scale (STSSS), the Yale Global Tic Severity Scale (YGTSS), the self-rated Tourette Syndrome Symptom List (TSSL), and a videotape-based rating scale.
RESULTS: Seven patients dropped out of the study or had to be excluded, but only 1 due to side effects. Using the TS-CGI, STSSS, YGTSS, and video rating scale, we found a significant difference (p <.05) or a trend toward a significant difference (p <.10) between THC and placebo groups at visits 2, 3, and/or 4. Using the TSSL at 10 treatment days (between days 16 and 41) there was a significant difference (p <.05) between both groups. ANOVA as well demonstrated a significant difference (p =.037). No serious adverse effects occurred.
CONCLUSION: Our results provide more evidence that THC is effective and safe in the treatment of tics. It, therefore, can be hypothesized that the central cannabinoid receptor system might play a role in TS pathology. (https://www.ncbi.nlm.nih.gov/pubmed/12716250)
Cannabinoids: possible role in pathophysiology and therapy of Gilles de la Tourette syndrome.
Müller-Vahl KR1, Kolbe H, Schneider U, Emrich HM. Author information
Abstract
High densities of cannabinoid receptors were found in the basal ganglia and hippocampus, indicating a putative functional role of cannabinoids in movement and behaviour. Anecdotal reports suggested beneficial effects of marijuana in Tourette's syndrome (TS). We therefore interviewed 64 TS patients with regard to use of marijuana and its influence on TS symptomatology. Of 17 patients (27%) who reported prior use of marijuana, 14 subjects (82%) experienced a reduction or complete remission of motor and vocal tics and an amelioration of premonitory urges and obsessive-compulsive symptoms. Our results provide more evidence that marijuana improves tics and behavioural disorders in TS. It can be speculated that cannabinoids might act through specific receptors, and that the cannabinoid system might play a major role in TS pathology. (https://www.ncbi.nlm.nih.gov/pubmed/9879795)
Article: Cannabis and Tourette Syndrome By Dustin Sulak, DO
(Dustin Sulak, D.O. is a renowned integrative medicine physician based in Maine, whose practice balances the principles of osteopathy, mind-body medicine and medical cannabis. Regarded as an expert on medical cannabis nationally, Dr. Sulak educates medical providers and patients on its clinical use, while continuing to explore the therapeutic potential of this ancient yet emerging medicine.)
Dr. Sulak received undergraduate degrees in nutrition science and biology from Indiana University, a doctorate of osteopathy from the Arizona College of Osteopathic Medicine, and completed an internship at Maine-Dartmouth Family Medicine Residency.
Tourette Syndrome is a common genetic neurological disorder characterized by chronic motor and vocal tics. Affected individuals typically have repetitive, stereotyped movements or vocalizations, such as blinking, sniffing, facial movements, or tensing of the abdomen.
Other manifestations include attention-deficit-hyperactivity disorder, obsessive-compulsive disorder, poor impulse control, and other behavioral problems. Symptoms vary significantly from one patient to another, and the tics are often not the most disabling features of this condition.
While the mechanism of Tourette syndrome remains unknown, research suggests that it is an inherited, developmental disorder of neurotransmission. This disorder affects approximately 1% of the population, and is 5 times more common in males. Symptoms range in severity from annoying to disabling.
Patients with loud vocalizations or large movements either endure substantial criticism or withdraw from many activities. Prejudice in work and school settings is common. Inadvertent injuries, such as broken bones and joint degeneration can also occur after years of simple yet repetitive tics. Accidents are common.
Current treatments of Tourette syndrome are purely symptomatic. No curative or preventive treatments are known. Medications have been used to treat tics, ADHD, OCD, and aggression. These include antipsychotics, dopamine-depleting agents, antihypertensive agents, skeletal muscle relaxants, benzodiazepines, SSRIs at 3-4 times the antidepressant dose, and Botox injections. Neurosurgery is performed in severe cases. All of these treatments carry significant risk and, sadly, offer limited benefit. Many medical authors encourage physicians avoid treating Tourette syndrome with pharmaceutical agents unless the symptoms are debilitating.
A significant body of scientific evidence suggests that the compounds found in cannabis can relieve symptoms of Tourette syndrome.
Animal studies demonstrate that cannabinoids specifically affect the basal ganglia and other areas of the brain known to be involved in Tourette syndrome.
Multiple case reports of patients using cannabis to reduce or eliminate tics and obsessive-compulsive behaviors have been published. One study found that cannabinoids could enhance the effectiveness of antipsychotic medications in this condition.
The randomized, double blind, placebo controlled trial is considered the gold standard in clinic trials for treatment efficacy. Two have been published that evaluated the efficacy of THC in the treatment of Tourette syndrome. The first, which included 12 adult patients, found that 10 of them experienced significant improvement in their symptoms after a single dose of THC, ranging from 20-90% reduction in symptom severity. Another study of 24 patients found similar improvements with no detrimental effects on cognition; verbal memory span actually improved in the cannabis group.
The acute effects of cannabis and THC are well documented, and are considered safer than most of the medications currently used in the treatment of Tourette syndrome. The lethal dose of cannabis and THC in humans is unknown and there are no reported deaths caused directly by cannabis toxicity.
I have personally seen cannabis help in debilitating cases of Tourette syndrome, after other medications had failed.
I would like to share a personal story. My best friend during ages 10-14, gradually developed Tourette syndrome right before my eyes. At first doctors thought he had postnasal drip or acid reflux. Over time, we joked that he was a one-man orchestra. The tics and obsessive-compulsive behavior worsened; the whole family suffered, and eventually he was no longer able to effectively function in a mainstream school environment. He left high school midway through freshman year and moved to a special needs school that was mostly attended by youth criminals. Our friendship quickly dissolved as he also became involved in delinquent activity.
Three years later I saw him and he was apparently tick-free. He confided in me that he had been introduced to marijuana by friends at his new school, and to his surprise, his symptoms had almost completely vanished after smoking. He went on to become a college graduate and successful salesman, an unlikely profession for someone with Tourette syndrome. This was the first case of effective medical cannabis usage I ever observed.
[http://healer.com/cannabis-and-tourette-syndrome/]
(Dustin Sulak, D.O. is a renowned integrative medicine physician based in Maine, whose practice balances the principles of osteopathy, mind-body medicine and medical cannabis. Regarded as an expert on medical cannabis nationally, Dr. Sulak educates medical providers and patients on its clinical use, while continuing to explore the therapeutic potential of this ancient yet emerging medicine.)
Dr. Sulak received undergraduate degrees in nutrition science and biology from Indiana University, a doctorate of osteopathy from the Arizona College of Osteopathic Medicine, and completed an internship at Maine-Dartmouth Family Medicine Residency.
Tourette Syndrome is a common genetic neurological disorder characterized by chronic motor and vocal tics. Affected individuals typically have repetitive, stereotyped movements or vocalizations, such as blinking, sniffing, facial movements, or tensing of the abdomen.
Other manifestations include attention-deficit-hyperactivity disorder, obsessive-compulsive disorder, poor impulse control, and other behavioral problems. Symptoms vary significantly from one patient to another, and the tics are often not the most disabling features of this condition.
While the mechanism of Tourette syndrome remains unknown, research suggests that it is an inherited, developmental disorder of neurotransmission. This disorder affects approximately 1% of the population, and is 5 times more common in males. Symptoms range in severity from annoying to disabling.
Patients with loud vocalizations or large movements either endure substantial criticism or withdraw from many activities. Prejudice in work and school settings is common. Inadvertent injuries, such as broken bones and joint degeneration can also occur after years of simple yet repetitive tics. Accidents are common.
Current treatments of Tourette syndrome are purely symptomatic. No curative or preventive treatments are known. Medications have been used to treat tics, ADHD, OCD, and aggression. These include antipsychotics, dopamine-depleting agents, antihypertensive agents, skeletal muscle relaxants, benzodiazepines, SSRIs at 3-4 times the antidepressant dose, and Botox injections. Neurosurgery is performed in severe cases. All of these treatments carry significant risk and, sadly, offer limited benefit. Many medical authors encourage physicians avoid treating Tourette syndrome with pharmaceutical agents unless the symptoms are debilitating.
A significant body of scientific evidence suggests that the compounds found in cannabis can relieve symptoms of Tourette syndrome.
Animal studies demonstrate that cannabinoids specifically affect the basal ganglia and other areas of the brain known to be involved in Tourette syndrome.
Multiple case reports of patients using cannabis to reduce or eliminate tics and obsessive-compulsive behaviors have been published. One study found that cannabinoids could enhance the effectiveness of antipsychotic medications in this condition.
The randomized, double blind, placebo controlled trial is considered the gold standard in clinic trials for treatment efficacy. Two have been published that evaluated the efficacy of THC in the treatment of Tourette syndrome. The first, which included 12 adult patients, found that 10 of them experienced significant improvement in their symptoms after a single dose of THC, ranging from 20-90% reduction in symptom severity. Another study of 24 patients found similar improvements with no detrimental effects on cognition; verbal memory span actually improved in the cannabis group.
The acute effects of cannabis and THC are well documented, and are considered safer than most of the medications currently used in the treatment of Tourette syndrome. The lethal dose of cannabis and THC in humans is unknown and there are no reported deaths caused directly by cannabis toxicity.
I have personally seen cannabis help in debilitating cases of Tourette syndrome, after other medications had failed.
I would like to share a personal story. My best friend during ages 10-14, gradually developed Tourette syndrome right before my eyes. At first doctors thought he had postnasal drip or acid reflux. Over time, we joked that he was a one-man orchestra. The tics and obsessive-compulsive behavior worsened; the whole family suffered, and eventually he was no longer able to effectively function in a mainstream school environment. He left high school midway through freshman year and moved to a special needs school that was mostly attended by youth criminals. Our friendship quickly dissolved as he also became involved in delinquent activity.
Three years later I saw him and he was apparently tick-free. He confided in me that he had been introduced to marijuana by friends at his new school, and to his surprise, his symptoms had almost completely vanished after smoking. He went on to become a college graduate and successful salesman, an unlikely profession for someone with Tourette syndrome. This was the first case of effective medical cannabis usage I ever observed.
[http://healer.com/cannabis-and-tourette-syndrome/]
Article: Cannabis can help improve symptoms of ADHD, according to the results of a new study.
Many people with attention deficit hyperactivity disorder (ADHD) find marijuana helpful for managing their symptoms, such as trouble focusing and being impulsive. But few studies have looked at marijuana as a treatment option, until now.
In a 2016 study by researchers at King’s College London, treatment with a cannabis-based spray was shown to reduce symptoms in patients with ADHD. The study involved 30 adults with ADHD, who were given either Sativex or placebo over a four-week period.
Sativex is a pharmaceutical spray made from extracts of the whole cannabis plant. It contains a 1:1 ratio of THC and CBD and is one of the very few cannabis-based treatments to be approved as a prescription drug.
By the end of the study, those who received cannabis treatment showed improvements in symptoms of hyperactivity, impulsivity and inattention. They also scored higher on measures of cognitive performance and emotional stability.
The researchers concluded: “ADHD may represent a subgroup of individuals that gain cognitive enhancement and reduction of ADHD symptoms from the use of cannabinoids.”
Cannabinoids are the active compounds in marijuana that are responsible for its medical properties. While over 80 different cannabinoids are known to exist, THC and CBD are the most common.
Both THC and CBD have been shown to improve ADHD symptoms in animal models.
Though cannabinoids are available in pharmaceutical forms like Sativex, many people with ADHD find marijuana to be an effective, more accessible option.
Marijuana Use and ADHD
The use of marijuana is extremely common in those who suffer from ADHD. In fact, studies show that young adults with ADHD are three times more likely to use marijuana in their lifetime.
While marijuana is usually seen as a recreational drug, people with ADHD often use marijuana as a way of self-medicating their symptoms.
In a study of 268 separate online discussions, 25% of people said they believed that marijuana was useful for treating ADHD.
Despite the popular belief that marijuana can help ADHD, how it works is still unclear.
People with ADHD are usually prescribed stimulant medications, such as Ritalin or Adderall, to help them focus and be less impulsive. These medications work by boosting dopamine levels in the brain.
Marijuana has also been shown to increase dopamine levels. This has led experts to theorize that marijuana might work in a similar way as stimulants in treating ADHD.
It also explains why some people find cannabis to be just as effective as their prescription medications. Compared to stimulants, marijuana is reported to have less side effects.
Many people with attention deficit hyperactivity disorder (ADHD) find marijuana helpful for managing their symptoms, such as trouble focusing and being impulsive. But few studies have looked at marijuana as a treatment option, until now.
In a 2016 study by researchers at King’s College London, treatment with a cannabis-based spray was shown to reduce symptoms in patients with ADHD. The study involved 30 adults with ADHD, who were given either Sativex or placebo over a four-week period.
Sativex is a pharmaceutical spray made from extracts of the whole cannabis plant. It contains a 1:1 ratio of THC and CBD and is one of the very few cannabis-based treatments to be approved as a prescription drug.
By the end of the study, those who received cannabis treatment showed improvements in symptoms of hyperactivity, impulsivity and inattention. They also scored higher on measures of cognitive performance and emotional stability.
The researchers concluded: “ADHD may represent a subgroup of individuals that gain cognitive enhancement and reduction of ADHD symptoms from the use of cannabinoids.”
Cannabinoids are the active compounds in marijuana that are responsible for its medical properties. While over 80 different cannabinoids are known to exist, THC and CBD are the most common.
Both THC and CBD have been shown to improve ADHD symptoms in animal models.
Though cannabinoids are available in pharmaceutical forms like Sativex, many people with ADHD find marijuana to be an effective, more accessible option.
Marijuana Use and ADHD
The use of marijuana is extremely common in those who suffer from ADHD. In fact, studies show that young adults with ADHD are three times more likely to use marijuana in their lifetime.
While marijuana is usually seen as a recreational drug, people with ADHD often use marijuana as a way of self-medicating their symptoms.
In a study of 268 separate online discussions, 25% of people said they believed that marijuana was useful for treating ADHD.
Despite the popular belief that marijuana can help ADHD, how it works is still unclear.
People with ADHD are usually prescribed stimulant medications, such as Ritalin or Adderall, to help them focus and be less impulsive. These medications work by boosting dopamine levels in the brain.
Marijuana has also been shown to increase dopamine levels. This has led experts to theorize that marijuana might work in a similar way as stimulants in treating ADHD.
It also explains why some people find cannabis to be just as effective as their prescription medications. Compared to stimulants, marijuana is reported to have less side effects.
Marijuana Helps Manage Symptoms
The reason why most people with ADHD use marijuana is better focus. Indeed, many find that cannabis helps them pay attention and stay on task.
This seems counter-intuitive, since marijuana is thought to interfere with focus and attention in regular users.
However, there are many other reasons why people with ADHD might choose to use marijuana. Besides being able to focus better, studies also suggest that marijuana can help with sleep difficulties, hyperactivity and being impulsive.
Interestingly, studies show that people with the most severe symptoms of ADHD tend to use marijuana more frequently. Men and women also appear to use cannabis for different reasons.
Despite the strong link between marijuana use and ADHD, more research is necessary to determine the specific benefits of marijuana in treating the condition.
Medical Marijuana For ADHD
Medical marijuana is becoming more popular in the U.S. and worldwide. It can be used to treat many conditions, including cancer, multiple sclerosis, chronic pain, Crohn’s disease and epilepsy.
Though using medical marijuana to treat ADHD is not widely accepted, some doctors support the idea.
“I had a patient who credited graduating with his use of marijuana. And I had a PhD candidate who credited marijuana with being able to get his PhD, and that’s because it helped him concentrate,” says Dr. Bearman, a physician in California who regularly prescribes marijuana to patients with ADHD.
David Bearman, M.D. Explains the Positive Relationship Between ADD/ADHD and Medical Cannabis
https://youtu.be/BXBbZ3O1jFY
Anxiety Disorder
While all human beings experience anxiety throughout their lives, Anxiety Disorders are a set of mental illnesses characterized by chronic and overwhelming emotions of fear, anxiousness, restlessness, and crippling worrying.
Examples of Anxiety Disorders include: Panic Disorder (which may cause complications of the heart); Social Anxiety Disorder; Selective Mutism (an inability to speak during specific but otherwise normal situations); various Phobias; Agoraphobia; Anxiety associated with Post Traumatic Stress Disorder (PTSD); Substance Induced Anxiety (alcohol abuse; drug abuse; opiate abuse; and even medication induced); and Generalized Anxiety Disorders which run the gamut of social hangups; disproportionate thinking; unhealthy obsessions; and so on.
These ailments are very debilitating and they are a major obstacle that sufferers face preventing them from leading a normal life. Resulting symptoms of these disorders include: problems with sleeping (insomnia); excessive sweating; irrational panicking; physical numbness; dizziness and nausea; heart palpitations; an inability to stay still and stay calm; painful muscle tensions and cramps; shortness of breath; and an inability to act or perform simple tasks.
Anxiety is a normal human emotion that everyone experiences at times. Many people feel anxious, or nervous, when faced with a problem at work, before taking a test, or making an important decision. Anxiety disorders, however, are different. They can cause such distress that it interferes with a person’s ability to lead a normal life. An anxiety disorder is a serious mental illness. For people with anxiety disorders, worry and fear are constant and overwhelming, and can be crippling.
Anxiety Disorders may either be developed through significant stressful incidents or situations in a sufferer’s life, or they may be hereditary. Thankfully, there are numerous therapies and medications that may help an individual treat and possibly rid themselves of their disorder.
Using Cannabis to Treat Anxiety Disorders
Cannabis is a complex medicinal plant that may actually be used to treat a variety of debilitating symptoms caused by a surprisingly large number of ailments. It’s usefulness as a non-lethal medicine (you cannot die from an overdose of cannabis) cannot be overstated and it’s versatility in terms of how it can be consumed and as to how it can be useful for so many illnesses is something to be excited about. However, it is important to remember that consulting with your primary care physician should be your first priority when considering incorporating cannabis into one’s medical regiment and that cannabis is to be used as an adjunct therapy and not a replacement. It is also your responsibility to communicate with your doctor as to how your use of cannabis has affected your health and of your progress with utilizing medical cannabis.
Currently, much of the ongoing research regarding cannabis’ ability to help with reducing anxiety has been focused on the powerful anxiolytic (anti-anxiety and anti-panic) properties of Cannabidiol (CBD). Overall, exciting studies have shown that cannabis may be quite useful for treating individuals suffering from Anxiety Disorders for the following reasons: significantly reducing anxiety itself; helping to manage possible depression associated with the anxiety disorder; helping to reduce nausea during a panic attack; assisting with sleep should the anxiety disorder cause insomnia; and with preventing possible psychosis.
Study: Cannabinoid Therapies May Help Treat Stress-Induced Anxiety Disorders
Cannabis is considered by many people to be a natural source of stress relief. In fact, an Israeli study published last year validates this claim, suggesting that “cannabinoid system activation could represent a novel approach to the treatment of cognitive deficits that accompany a variety of stress-related neuropsychiatric disorders.”
Hoping to expand on these findings, a team of researchers from Vanderbilt University in Tennessee published a study in a issue of Translational Psychiatry. Their results suggest that increasing one’s levels of endocannabinoids, particularly anandamide, could be a viable treatment for stress-induced anxiety.
What Is Anandamide?
Anandamide is an endocannabinoid, which means our body produces it naturally. It operates in a similar manner to tetrahydrocannabinol (THC) and effects the CB1 receptors as well as the CB2 receptors.
Past research has shown that anandamide can fight against human breast cancer and aggressive skin cancer, among other benefits. It is also likely that anandamide plays a role in many of the benefits offered by cannabidiol (CBD), considering the fact that CBD inhibits the production of fatty acid amide hydrolase (FAAH), an enzyme that degrades anandamide.
A few months ago, we published a piece about the apparent relationship between CBD and social anxiety. However, the study offered little evidence as to the mechanisms underlying the cannabinoid benefits.
That being said, it’s entirely possible that anandamide was responsible for the significant improvement in anxiety experienced by patients in the previous study. The research performed at Vanderbilt University seems to increase the likelihood of this hypothesis.
Increased Anandamide May Help Treat Stress-Induced Anxiety
In order to test the relationship between anandamide and stress-induced anxiety, the Vanderbilt research team conducted a series of tests using mice as subjects. First, they shocked the mice’s feet six times for two seconds each to induce stress – there was a one-minute interval between each shock.
24 hours later, the mice were subjected to a number of behavioral assays to determine whether this foot-shock would result in an anxious response. The results of two different tests suggested that the mice were in fact dealing with anxiety, according to the research team.
“The endocannabinoid was able to reverse the stress-induced state of anxiety in mice.”
In an attempt to counter the effects of this anxiety, the researchers administered an inhibitor of fatty acid amide hydrolase (FAAH) to prevent the enzyme from degrading anandamide. Their results suggest that the endocannabinoid was able to reverse the stress-induced state of anxiety in mice.
How Can Medical Cannabis Help Treat Stress And Anxiety?
Perhaps more interesting, the Vanderbilt research team reported that anandamide levels throughout the brain were reduced 24 hours after shocking the mice’s feet. This was negatively-correlated with their experience of anxiety (more anandamide = less anxiety), which lead researchers to the conclusion that “central anandamide levels predict acute stress-induced anxiety.”
The Vanderbilt research team explains that their findings “strongly support the utility of anandamide augmentation as a therapeutic approach for stress-related affective and anxiety disorders.”
Considering that cannabidiol (CBD) can inhibit the degradation of anandamide and tetrahydrocannabinol (THC) can mimic its effects, one can reasonably infer that cannabis-based therapies may help counter stress-induced anxiety. Of course, more research will be necessary to verify the effectiveness of such treatments.
Study: Cannabidiol (CBD) May Help Treat Social Anxiety Disorder
The relationship between cannabis and anxiety is an interesting one. Large concentrations of tetrahydrocannabinol (THC) is often tied to bouts of paranoia and anxiety, however it is well-documented that cannabidiol (CBD) found in cannabis can counteract this effect.
With that said, a group of Brazilian researchers published an article in the 2011 Journal of Psychopharmacology that further investigates the relationship between cannabidiol (CBD) and Social Anxiety Disorder (SAD). Their results suggest that CBD could offer a way for people suffering from SAD to help manage their symptoms.
What Is Social Anxiety Disorder (SAD)?
Affecting 12% of Americans in their lifetime, Social Anxiety Disorder (SAD) is the most common form of anxiety and one of the most psychiatric disorders in general. It is also referred to as social phobia.
By definition, Social Anxiety Disorder is characterized by intense fear in one or more social situations. In turn, this fear can cause distress to the point that it impairs daily functioning.
Interestingly enough, people who suffer from SAD experience anxiety that can be triggered by “perceived or actual scrutiny” from others. For some this only happens in specific situations, but others may have to deal with this anxiety constantly.
Brazilian Researchers Investigate CBD, Anxiety In Humans
In order to test the relationship between cannabidiol (CBD) and anxiety, the Brazilian research team recruited 10 people with a diagnosis of Social Anxiety Disorder (SAD). They then used functional neuroimaging to gauge the amount of blood flow in various parts of the brain, noting the effects of CBD.
In the first session, half received an oral dose of 400 mg of cannabidiol (CBD) and the other half were treated with placebos. These roles were reversed in the second session so that all 10 participants were treated with CBD at some point.
“These results suggest that CBD reduces anxiety in SAD and that this is related to its effects on activity in limbic and paralimbic brain areas.” – Dr. J.A. Crippa
According to the results of the study, cannabidiol (CBD) was associated with a significant decrease in subjective anxiety. Cerebral blood flow after CBD treatment also seems to point to an anxiolytic (anti-anxiety) effect in the areas of the brain that control emotions.
Expanding on what this could all mean is Dr. J. A. Crippa, who led the Brazilian research team. “These results suggest that CBD reduces anxiety in SAD and that this is related to its effects on activity in limbic and paralimbic brain areas,” Crippa explains.
Prescription Pills:
Each year, about 4.5 million Americans visit their doctor’s office or the emergency room because of adverse prescription drug side effects. A startling 2 million other patients who are already hospitalized suffer the ill effects of prescription medications annually, and this when they should be under the watchful eye of medical professionals. The most common non-severe or mild side effects from taking drugs include (there are many more, these are the most common): Constipation, Dermatitis, Diarrhea, Dizziness, Drowsiness, Dry mouth, Headache, and Insomnia.
What are the short and long term effects of prescription drugs? Short-term effects: Alertness, focus, sleeplessness, loss of appetite, increased blood pressure and heart rate, high body temperature.
Long-term effects: Addiction, paranoia and long-term insomnia, extreme weight change.
What are the effects of prescription drugs? Physical symptoms: Increased or decreased need for sleep, Appearing unusually energetic, or overly fatigued, Increased or decreased appetite.
These drugs come with side effects that range from birth defects and liver damage to suicidal behavior, blood clots, bladder cancer, Crohn’s disease, heart attacks, strokes, uncontrollable bleeding, heart failure and death: Chronic Pain Treatment drug Fentanyl (opioid). Type 2 diabetes drugs Avandia and Actos. Antidepressants Paxil, Prozac, Effexor, Zoloft and Lexapro. Mood stabilizer Depakote. Birth control pills Yaz and Yasmin. Acne medication Accutane. Blood thinners Pradaxa and Xarelto Osteoporosis treatment Fosamax. GranuFlo and NaturaLyte, which are used in dialysis.
Hair loss pill Propecia. Stop smoking cigarettes drug Chantix.
In article in American-Statesman staff writer Jeremy Schwartz in 2012 noted that in 2011, “the Pentagon spent more on pills, injections and vaccines than it did on Black Hawk helicopters, Abrams tanks, Hercules C-130 cargo planes and Patriot missiles — combined.” The military spent at least $2.7 billion on antidepressants and more than $1.6 billion on opioid painkillers such as Oxycontin and hydrocodone over the past decade. More than $507 million was spent on the sleeping pill Ambien and its generic equivalents.” the pharmaceutical industry spent about $1.7 million for more than 1,400 trips for Defense Department doctors and pharmacists to places such as Paris, Las Vegas and New Orleans between 1998 and 2007. All those Pills killed a lot of Veterans, Cannabis has a 5000 year history with zero deaths associated with it.
These ailments are very debilitating and they are a major obstacle that sufferers face preventing them from leading a normal life. Resulting symptoms of these disorders include: problems with sleeping (insomnia); excessive sweating; irrational panicking; physical numbness; dizziness and nausea; heart palpitations; an inability to stay still and stay calm; painful muscle tensions and cramps; shortness of breath; and an inability to act or perform simple tasks.
Anxiety is a normal human emotion that everyone experiences at times. Many people feel anxious, or nervous, when faced with a problem at work, before taking a test, or making an important decision. Anxiety disorders, however, are different. They can cause such distress that it interferes with a person’s ability to lead a normal life. An anxiety disorder is a serious mental illness. For people with anxiety disorders, worry and fear are constant and overwhelming, and can be crippling.
Anxiety Disorders may either be developed through significant stressful incidents or situations in a sufferer’s life, or they may be hereditary. Thankfully, there are numerous therapies and medications that may help an individual treat and possibly rid themselves of their disorder.
Using Cannabis to Treat Anxiety Disorders
Cannabis is a complex medicinal plant that may actually be used to treat a variety of debilitating symptoms caused by a surprisingly large number of ailments. It’s usefulness as a non-lethal medicine (you cannot die from an overdose of cannabis) cannot be overstated and it’s versatility in terms of how it can be consumed and as to how it can be useful for so many illnesses is something to be excited about. However, it is important to remember that consulting with your primary care physician should be your first priority when considering incorporating cannabis into one’s medical regiment and that cannabis is to be used as an adjunct therapy and not a replacement. It is also your responsibility to communicate with your doctor as to how your use of cannabis has affected your health and of your progress with utilizing medical cannabis.
Currently, much of the ongoing research regarding cannabis’ ability to help with reducing anxiety has been focused on the powerful anxiolytic (anti-anxiety and anti-panic) properties of Cannabidiol (CBD). Overall, exciting studies have shown that cannabis may be quite useful for treating individuals suffering from Anxiety Disorders for the following reasons: significantly reducing anxiety itself; helping to manage possible depression associated with the anxiety disorder; helping to reduce nausea during a panic attack; assisting with sleep should the anxiety disorder cause insomnia; and with preventing possible psychosis.
Study: Cannabinoid Therapies May Help Treat Stress-Induced Anxiety Disorders
Cannabis is considered by many people to be a natural source of stress relief. In fact, an Israeli study published last year validates this claim, suggesting that “cannabinoid system activation could represent a novel approach to the treatment of cognitive deficits that accompany a variety of stress-related neuropsychiatric disorders.”
Hoping to expand on these findings, a team of researchers from Vanderbilt University in Tennessee published a study in a issue of Translational Psychiatry. Their results suggest that increasing one’s levels of endocannabinoids, particularly anandamide, could be a viable treatment for stress-induced anxiety.
What Is Anandamide?
Anandamide is an endocannabinoid, which means our body produces it naturally. It operates in a similar manner to tetrahydrocannabinol (THC) and effects the CB1 receptors as well as the CB2 receptors.
Past research has shown that anandamide can fight against human breast cancer and aggressive skin cancer, among other benefits. It is also likely that anandamide plays a role in many of the benefits offered by cannabidiol (CBD), considering the fact that CBD inhibits the production of fatty acid amide hydrolase (FAAH), an enzyme that degrades anandamide.
A few months ago, we published a piece about the apparent relationship between CBD and social anxiety. However, the study offered little evidence as to the mechanisms underlying the cannabinoid benefits.
That being said, it’s entirely possible that anandamide was responsible for the significant improvement in anxiety experienced by patients in the previous study. The research performed at Vanderbilt University seems to increase the likelihood of this hypothesis.
Increased Anandamide May Help Treat Stress-Induced Anxiety
In order to test the relationship between anandamide and stress-induced anxiety, the Vanderbilt research team conducted a series of tests using mice as subjects. First, they shocked the mice’s feet six times for two seconds each to induce stress – there was a one-minute interval between each shock.
24 hours later, the mice were subjected to a number of behavioral assays to determine whether this foot-shock would result in an anxious response. The results of two different tests suggested that the mice were in fact dealing with anxiety, according to the research team.
“The endocannabinoid was able to reverse the stress-induced state of anxiety in mice.”
In an attempt to counter the effects of this anxiety, the researchers administered an inhibitor of fatty acid amide hydrolase (FAAH) to prevent the enzyme from degrading anandamide. Their results suggest that the endocannabinoid was able to reverse the stress-induced state of anxiety in mice.
How Can Medical Cannabis Help Treat Stress And Anxiety?
Perhaps more interesting, the Vanderbilt research team reported that anandamide levels throughout the brain were reduced 24 hours after shocking the mice’s feet. This was negatively-correlated with their experience of anxiety (more anandamide = less anxiety), which lead researchers to the conclusion that “central anandamide levels predict acute stress-induced anxiety.”
The Vanderbilt research team explains that their findings “strongly support the utility of anandamide augmentation as a therapeutic approach for stress-related affective and anxiety disorders.”
Considering that cannabidiol (CBD) can inhibit the degradation of anandamide and tetrahydrocannabinol (THC) can mimic its effects, one can reasonably infer that cannabis-based therapies may help counter stress-induced anxiety. Of course, more research will be necessary to verify the effectiveness of such treatments.
Study: Cannabidiol (CBD) May Help Treat Social Anxiety Disorder
The relationship between cannabis and anxiety is an interesting one. Large concentrations of tetrahydrocannabinol (THC) is often tied to bouts of paranoia and anxiety, however it is well-documented that cannabidiol (CBD) found in cannabis can counteract this effect.
With that said, a group of Brazilian researchers published an article in the 2011 Journal of Psychopharmacology that further investigates the relationship between cannabidiol (CBD) and Social Anxiety Disorder (SAD). Their results suggest that CBD could offer a way for people suffering from SAD to help manage their symptoms.
What Is Social Anxiety Disorder (SAD)?
Affecting 12% of Americans in their lifetime, Social Anxiety Disorder (SAD) is the most common form of anxiety and one of the most psychiatric disorders in general. It is also referred to as social phobia.
By definition, Social Anxiety Disorder is characterized by intense fear in one or more social situations. In turn, this fear can cause distress to the point that it impairs daily functioning.
Interestingly enough, people who suffer from SAD experience anxiety that can be triggered by “perceived or actual scrutiny” from others. For some this only happens in specific situations, but others may have to deal with this anxiety constantly.
Brazilian Researchers Investigate CBD, Anxiety In Humans
In order to test the relationship between cannabidiol (CBD) and anxiety, the Brazilian research team recruited 10 people with a diagnosis of Social Anxiety Disorder (SAD). They then used functional neuroimaging to gauge the amount of blood flow in various parts of the brain, noting the effects of CBD.
In the first session, half received an oral dose of 400 mg of cannabidiol (CBD) and the other half were treated with placebos. These roles were reversed in the second session so that all 10 participants were treated with CBD at some point.
“These results suggest that CBD reduces anxiety in SAD and that this is related to its effects on activity in limbic and paralimbic brain areas.” – Dr. J.A. Crippa
According to the results of the study, cannabidiol (CBD) was associated with a significant decrease in subjective anxiety. Cerebral blood flow after CBD treatment also seems to point to an anxiolytic (anti-anxiety) effect in the areas of the brain that control emotions.
Expanding on what this could all mean is Dr. J. A. Crippa, who led the Brazilian research team. “These results suggest that CBD reduces anxiety in SAD and that this is related to its effects on activity in limbic and paralimbic brain areas,” Crippa explains.
Prescription Pills:
Each year, about 4.5 million Americans visit their doctor’s office or the emergency room because of adverse prescription drug side effects. A startling 2 million other patients who are already hospitalized suffer the ill effects of prescription medications annually, and this when they should be under the watchful eye of medical professionals. The most common non-severe or mild side effects from taking drugs include (there are many more, these are the most common): Constipation, Dermatitis, Diarrhea, Dizziness, Drowsiness, Dry mouth, Headache, and Insomnia.
What are the short and long term effects of prescription drugs? Short-term effects: Alertness, focus, sleeplessness, loss of appetite, increased blood pressure and heart rate, high body temperature.
Long-term effects: Addiction, paranoia and long-term insomnia, extreme weight change.
What are the effects of prescription drugs? Physical symptoms: Increased or decreased need for sleep, Appearing unusually energetic, or overly fatigued, Increased or decreased appetite.
These drugs come with side effects that range from birth defects and liver damage to suicidal behavior, blood clots, bladder cancer, Crohn’s disease, heart attacks, strokes, uncontrollable bleeding, heart failure and death: Chronic Pain Treatment drug Fentanyl (opioid). Type 2 diabetes drugs Avandia and Actos. Antidepressants Paxil, Prozac, Effexor, Zoloft and Lexapro. Mood stabilizer Depakote. Birth control pills Yaz and Yasmin. Acne medication Accutane. Blood thinners Pradaxa and Xarelto Osteoporosis treatment Fosamax. GranuFlo and NaturaLyte, which are used in dialysis.
Hair loss pill Propecia. Stop smoking cigarettes drug Chantix.
In article in American-Statesman staff writer Jeremy Schwartz in 2012 noted that in 2011, “the Pentagon spent more on pills, injections and vaccines than it did on Black Hawk helicopters, Abrams tanks, Hercules C-130 cargo planes and Patriot missiles — combined.” The military spent at least $2.7 billion on antidepressants and more than $1.6 billion on opioid painkillers such as Oxycontin and hydrocodone over the past decade. More than $507 million was spent on the sleeping pill Ambien and its generic equivalents.” the pharmaceutical industry spent about $1.7 million for more than 1,400 trips for Defense Department doctors and pharmacists to places such as Paris, Las Vegas and New Orleans between 1998 and 2007. All those Pills killed a lot of Veterans, Cannabis has a 5000 year history with zero deaths associated with it.
“Its margin of safety is immense and underscores the lack of any meaningful danger in using not only daily doses in the 3.5 – 9 gram range, but also considerably higher doses.”— David Bearman, M.D. (Physician, researcher, court-qualified cannabis expert)
Beneficial Cannabinoids and Terpenes Useful for Treating Anxiety Disorders
The cannabis plant offers a plethora of therapeutic benefits and contains cannabinoids and terpenoid compounds that are useful for treating some of the symptoms caused by an Anxiety Disorder. While much of the interest in treating an Anxiety Disorder with cannabis involves CBD, the following chart denotes which cannabinoids and terpenoids also work synergistically with each other for possible therapeutic benefit.
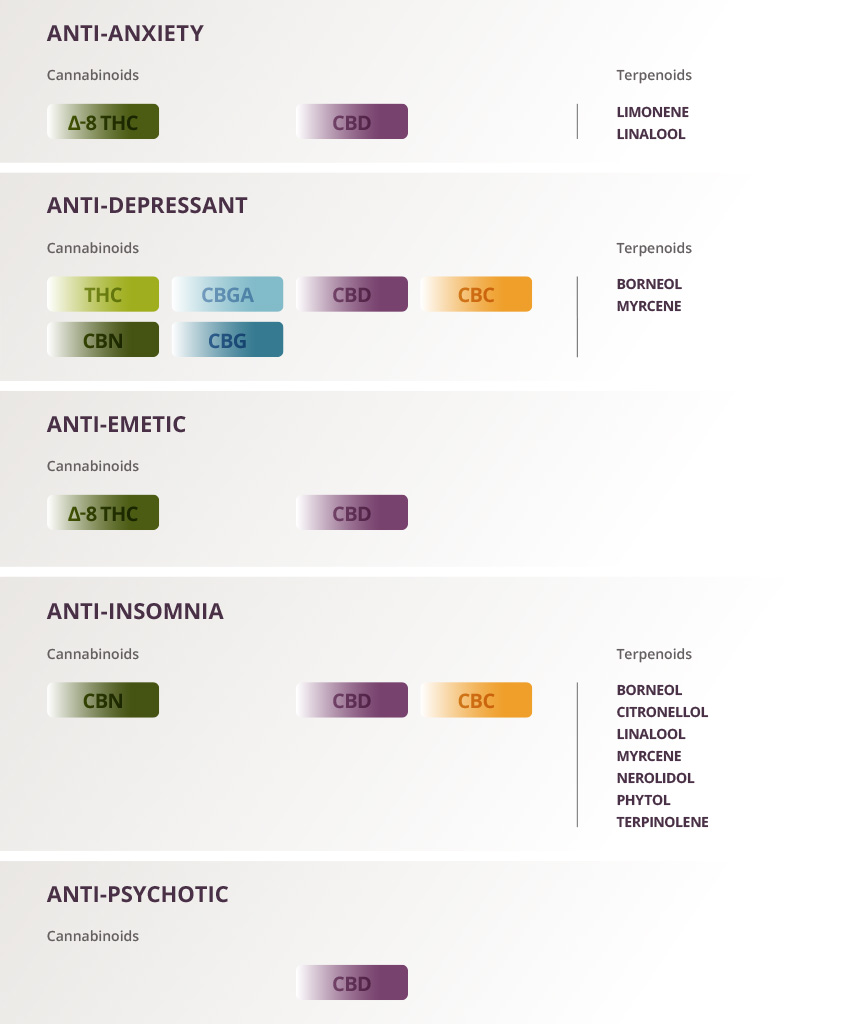 |
| Credit: Elemental Wellness |
Fear and anxiety are part of life. You may feel anxious before you take a test or walk down a dark street. This kind of anxiety is useful – it can make you more alert or careful. It usually ends soon after you are out of the situation that caused it. But for millions of people in the United States, the anxiety does not go away, and gets worse over time. Learn more about anxiety and Medical Cannabis; Information on Medical Cannabis treatments for Anxiety.
There is a wealth of new scientific understanding regarding how medical cannabis can be beneficial for treating Pain.
One person may suffer from strong anxiety attacks that strike without warning, while another gets panicky at the thought of speaking at an event. Someone else may struggle with a disabling fear of driving, or uncontrollable, intrusive thoughts. Yet another may live in a constant state of tension, worrying about anything and everything.
Types of Anxiety:
Anxiety and Medical Cannabis: Medical Cannabis Related Clinical Information
- Endocannabinoids and Stress
- Endocannabinoid-mediated modulation of stress responses: physiological and pathophysiological significance
- Cannabinoids ameliorate impairments induced by chronic stress to synaptic plasticity and short-term memory
Anxiety Research Showing How Medical Cannabis Is Beneficial
- Antidepressant-Like and Anxiolytic-Like Effects of Cannabidiol: A Chemical Compound of Cannabis Sativa [http://www.ncbi.nlm.nih.gov/pubmed/24923339]
- CBD reduces the anxiety induced by simulated public speaking in treatment-naïve social phobia patients [http://www.ncbi.nlm.nih.gov/pubmed/21307846]
- Neural basis of anxiolytic effects of CBD in generalized social anxiety disorder [http://www.ncbi.nlm.nih.gov/pubmed/20829306]
- Central anandamide deficiency predicts stress-induced anxiety: behavioral reversal through endocannabinoid augmentation [http://www.ncbi.nlm.nih.gov/pubmed/25004388]
- Effects of CBD on regional cerebral blood flow [http://www.ncbi.nlm.nih.gov/pubmed/14583744]
- The anxiolytic-like effects of cannabidiol injected into the bed nucleus of the stria terminalis are mediated by 5-HT1A receptors [http://www.ncbi.nlm.nih.gov/pubmed/20945065]
- Plant-based medicines for anxiety disorders, part 2 [http://www.ncbi.nlm.nih.gov/pubmed/23653088]
- A systematic review of plant-derived natural compounds for anxiety disorders [http://www.ncbi.nlm.nih.gov/pubmed/26845556]
Research: The Endocannabinoid System and Anxiety.
[Vitam Horm. 2017;103:193-279. doi: 10.1016/bs.vh.2016.09.006. Epub 2016 Nov 2.]
Lisboa SF1, Gomes FV2, Terzian AL3, Aguiar DC4, Moreira FA4, Resstel LB3, Guimarães FS5. Author information
Abstract
The medical properties of Cannabis sativa is known for centuries. Since the discovery and characterization of the endogenous cannabinoid system, several studies have evaluated how cannabinoid compounds and, particularly, how the modulation of the endocannabinoid (eCB) system influences a wide range of functions, from metabolic to mental disorders. Cannabinoids and eCB system often exert opposite effects on several functions, such as anxiety. Although the mechanisms are not completely understood, evidence points to different factors influencing those effects. In this chapter, the recent advances in research about the relationship between eCB system and anxiety disorders in humans, as well as in animal models, will be discussed. The recent data addressing modulation of the eCBs in specific brain areas, such as the medial prefrontal cortex, amygdaloid complex, bed nucleus of stria terminalis, hippocampus, and dorsal periaqueductal gray, will be summarized. Finally, data from animal models addressing the mechanisms through which the eCB system modulates anxiety-related behavior dependent on stressful situations, such as the involvement of different receptors, distinct eCBs, modulation of neurotransmitters release, HPA axis and immune system activation, and plastic mechanisms, will also be discussed.
Research: Cannabidiol, a Cannabis sativa constituent, as an anxiolytic drug.
[https://www.ncbi.nlm.nih.gov/pubmed/22729452]
Schier AR1, Ribeiro NP, Silva AC, Hallak JE, Crippa JA, Nardi AE, Zuardi AW.
Author information
Abstract
OBJECTIVES:
To review and describe studies of the non-psychotomimetic constituent of Cannabis sativa, cannabidiol (CBD), as an anxiolytic drug and discuss its possible mechanisms of action.
METHOD:
The articles selected for the review were identified through searches in English, Portuguese, and Spanish in the electronic databases ISI Web of Knowledge, SciELO, PubMed, and PsycINFO, combining the search terms "cannabidiol and anxiolytic", "cannabidiol and anxiolytic-like", and "cannabidiol and anxiety". The reference lists of the publications included, review articles, and book chapters were hand searched for additional references. Experimental animal and human studies were included, with no time restraints.
RESULTS:
Studies using animal models of anxiety and involving healthy volunteers clearly suggest an anxiolytic-like effect of CBD. Moreover, CBD was shown to reduce anxiety in patients with social anxiety disorder.
CONCLUSION:
Future clinical trials involving patients with different anxiety disorders are warranted, especially of panic disorder, obsessive-compulsive disorder, social anxiety disorder, and post-traumatic stress disorders. The adequate therapeutic window of CBD and the precise mechanisms involved in its anxiolytic action remain to be determined.
Research: Evidences for the Anti-panic Actions of Cannabidiol.
Soares VP, Campos AC1. [https://www.ncbi.nlm.nih.gov/pubmed/27157263]
Author information
Abstract
BACKGROUND:
Panic disorder (PD) is a disabling psychiatry condition that affects approximately 5% of the worldwide population. Currently, long-term selective serotonin reuptake inhibitors (SSRIs) are the first-line treatment for PD; however, the common side-effect profiles and drug interactions may provoke patients to abandon the treatment, leading to PD symptoms relapse. Cannabidiol (CBD) is the major non-psychotomimetic constituent of the Cannabis sativa plant with antianxiety properties that has been suggested as an alternative for treating anxiety disorders. The aim of the present review was to discuss the effects and mechanisms involved in the putative anti-panic effects of CBD.
METHODS:
electronic database was used as source of the studies selected selected based on the studies found by crossing the following keywords: cannabidiol and panic disorder; canabidiol and anxiety, cannabidiol and 5-HT1A receptor).
RESULTS:
In the present review, we included both experimental laboratory animal and human studies that have investigated the putative anti-panic properties of CBD. Taken together, the studies assessed clearly suggest an anxiolytic-like effect of CBD in both animal models and healthy volunteers.
CONCLUSIONS:
CBD seems to be a promising drug for the treatment of PD. However, novel clinical trials involving patients with the PD diagnosis are clearly needed to clarify the specific mechanism of action of CBD and the safe and ideal therapeutic doses of this compound.
Research: Cannabidiol reduces the anxiety induced by simulated public speaking in treatment-naïve social phobia patients.
Neuropsychopharmacology. 2011 May;36(6):1219-26. doi: 10.1038/npp.2011.6. Epub 2011 Feb 9.
Author information
Abstract
Generalized Social Anxiety Disorder (SAD) is one of the most common anxiety conditions with impairment in social life. Cannabidiol (CBD), one major non-psychotomimetic compound of the cannabis sativa plant, has shown anxiolytic effects both in humans and in animals. This preliminary study aimed to compare the effects of a simulation public speaking test (SPST) on healthy control (HC) patients and treatment-naïve SAD patients who received a single dose of CBD or placebo. A total of 24 never-treated patients with SAD were allocated to receive either CBD (600 mg; n=12) or placebo (placebo; n=12) in a double-blind randomized design 1 h and a half before the test. The same number of HC (n=12) performed the SPST without receiving any medication. Each volunteer participated in only one experimental session in a double-blind procedure. Subjective ratings on the Visual Analogue Mood Scale (VAMS) and Negative Self-Statement scale (SSPS-N) and physiological measures (blood pressure, heart rate, and skin conductance) were measured at six different time points during the SPST. The results were submitted to a repeated-measures analysis of variance. Pretreatment with CBD significantly reduced anxiety, cognitive impairment and discomfort in their speech performance, and significantly decreased alert in their anticipatory speech. The placebo group presented higher anxiety, cognitive impairment, discomfort, and alert levels when compared with the control group as assessed with the VAMS. The SSPS-N scores evidenced significant increases during the testing of placebo group that was almost abolished in the CBD group. No significant differences were observed between CBD and HC in SSPS-N scores or in the cognitive impairment, discomfort, and alert factors of VAMS. The increase in anxiety induced by the SPST on subjects with SAD was reduced with the use of CBD, resulting in a similar response as the HC.
References for Anxiety Disorder
- Diagnostic criteria for anxiety disorders set out in DSM-IV and ICD-10 classification systems
- Understanding Medical Cannabis.Elemental Wellness Center, 2014 Jul.
- Cannabidiol, a cannabis sativa constituent, as an anxiolytic drug.Schier, Alexandre de Mello, et al. Revista Brasileira de Psiquiatria, 2012 Jun, 34(1).
- Neural basis of anxiolytic effects of cannabidiol (CBD) in generalized social anxiety disorder: a preliminary report.Crippa, Jose Alexandre S., et al. Journal of Psychopharmacology, 2010 Sep 9, 25(1): 121-130.
- Chapter 5 the endocannabinoid system as a target for novel anxiolytic and antidepressant drugs.Gaetani, Silvana, et al. International Review of Neurobiology, 2009, 85: 57-72.
- Modulation of fear and anxiety by the endogenous cannabinoid system.Chhatwal, James P., et al. CNS spectrums, 2007 Mar, 12(3): 211-220.
- Effects of cannabinoids on the anxiety-like response in mice.Rutkowska, Maria, et al. Pharmacological Reports, 2006, 58: 200-206.
- Cannabidiol, a cannabis sativa constituent, as an antipsychotic drug.Zuardi, A.W., et al. Brazilian Journal of Medical and Biological Research, 2006 Apr, 39(4): 421-429.
- Pharmacological evaluation of cannabinoid receptor ligands in a mouse model of anxiety: further evidence for an anxiolytic role for endogenous cannabinoid signaling.Patel, Sachin, et al. Journal of Pharmacology and Experimental Therapeutics, 2006 Mar 28, 318(1): 304-311.
- Anxiolytic-like effect of cannabidiol in the rat vogel conflict test.Moreira, Fabricio A., et al. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 2006 Dec 30, 30(8): 1466-1471.
- Cannabinoids promote embryonic and adult hippocampus neurogenesis and produce anxiolytic- and antidepressant-like effects.Jiang, Wen, et al. The Journal of Clinical Investigation, 2005 Nov 1, 115(11): 3104-3116.
- A role for cannabinoid CB1 receptors in mood and anxiety disorders.Witkin, J.M., et al. Behavioral Pharmacology, 2005 Sep, 16(5-6): 315-331.
- Endocannabinoid system and stress and anxiety responses.Viveros, M.P., et al. Pharmacology Biochemistry and Behavior, 2005 Jun, 81(2): 331-342.
- Cannabis and cannabis extracts: greater than the sum of their parts.McPartland, John M., et al. Journal of Cannabis Therapeutics, 2001, 1(3-4): 103-32.
- Action of cannabidiol on the anxiety and other effects produced by Δ9-THC in normal subjects. Zuardi, A.W., et al. Psychopharmacology, 1982 Mar, 76(3): 245-250.
- The efficacy and safety of nabilone (a synthetic cannabinoid) in the treatment of anxiety. Fabre, Louis F., et al. The Journal of Clinical Pharmacology, 1981 Aug, 21(S1): 377-382.
Tourette's Continued:
FINDINGS: EFFECTS OF CANNABIS ON TOURETTE SYNDROME
Research has shown that cannabis can be effective in suppressing tics and also in the treatment of the syndrome’s associated behavioral problems (Muller-Vahl, 2013) (Abi-Jaoude, et al., 2017). One study measuring the effects of a single cannabis treatment on adult Tourette’s syndrome patients found a significant improvement of tics and obsessive-compulsive behavior compared to placebo (Muller-Vahl, et al., 2002). Demonstrating cannabis potential longer-term benefits, another study discovered a significant difference in the reduction of tics compared to placebo in Tourette’s patients after six weeks of cannabis administration (Muller-Vahl, et al., 2003). Another study, also involving six-weeks of cannabis treatments, reported a reduction tics in patients with Tourette’s with no serious adverse effects or impairment on neuropsychological performance (Muller-Vahl, 2003).
Tourette syndrome patients being treated with cannabis have shown to experience no impairments in verbal and visual memory, reaction time, intelligence, sustained attention, divided attention, vigilance or mood compared to placebo treatment (Muller-Vahl, et al., 2002). Therefore, regular cannabis use to manage the symptoms associated with Tourette’s appears to have no acute or long-term cognitive effects (Muller-Vahl, et al., 2003).
RECENT STUDIES ON CANNABIS’ EFFECT ON TOURETTE SYNDROME
Cannabis and cannabinoid therapy is increasingly being investigated and used in the treatment of a wide variety of pathologies with varying levels of success. While the efficacy of cannabis has been better studied and documented in the treatment of conditions such as epilepsy and glaucoma (Rosenberg et al., 2016; Tomida et al., 2004), other areas of cannabis research and medicine are still in its infancy and offer limited data.
One conditioning gaining popularity as a viable candidate for cannabinoid therapy is Attention Deficit Hyperactivity Disorder (ADHD). A new 2017 study performed by Cooper and colleagues piloted a randomized, placebo-controlled study involving the administration of Sativex, a whole plant cannabinoid medication, to 20 adults diagnosed with ADHD (Cooper et al., 2017). While the results of this study suggest the benefits of cannabis in the treatment of ADHD may be largely subjective, emerging data seems to suggest that the endocannabinoid system may be implicated in the pathophysiology of ADHD and should therefore be further investigated.
The mechanism for cannabinoids in the pathology of ADHD is still largely unknown, however, it is thought to be related to enhanced dopaminergic transmission (Cooper et al., 2017). This enhanced dopamine activity is the reason stimulants are considered the “gold standard” for pharmacotreatment of ADHD (Punja et al., 2016). Physicians, however, are sometimes reluctant to prescribe such psychotropic drugs to a population of patients commonly presenting with a comorbidity for substance abuse.
The same reluctance may be a factor in using cannabis, a widely abused drug, in the treatment of ADHD as well. However, this author argues that the side effect profile of cannabis may be better tolerated than that of stimulants. Insomnia is one of the most commonly reported side effects of stimulant medication and can have significantly detrimental effects on the patient, especially in children (Punja et al., 2016).
A 12-year comprehensive review showed a steep rise in stimulant medications (0.6% in 1987 to 2.7% in 1997) prescribed to children over time for the treatment of ADHD (Zuvekas & Vitiello, 2012). The use of these powerful psychotropic meds in children has begun to spur some controversy. A similar concern presents itself when considering cannabis treatment for ADHD in pediatric patients. More research is beginning to emerge on the role of cannabis in the developing brain and the results warrant further investigation into cannabis therapy in pediatric patients.
In trying to understand the role of cannabis use in the developing brain, it is critical to explore the documented neurocognitive effects of cannabis in children and adolescents. Recent attention has been brought to remarkably dramatic case reports of children with debilitating illnesses failing to respond to traditional medicine and for whom cannabis is the only solution. As such, there are an increasing number of pediatric and adolescent patients being added to the medical cannabis registry, particularly for conditions such as epilepsy (Handland et al., 2016).
According to highly specialized medical cannabis doctor Dr. Bonni Goldstein, ”There are many patients who suffer with Tourette syndrome (TS) who are finding relief of symptoms with cannabis.” Goldstein further added, “A large percentage of people who have been diagnosed with TS also suffer with other significant conditions, such as OCD, ADHD, mood disorders and anxiety. The conventional medications used to treat these conditions are not always helpful and often cause a wide array of unwanted side effects.”
Treating Adult ADHD with Cannabis
The Society of Cannabis Clinicians also states that; The medical certificates of 30 patients with adult ADHD, who were granted approval by the German Health Ministry to use cannabis flowers between 2012 and 2014, were analysed with regard to course of disease, previous treatment efforts, and effects of self-medication with cannabis or therapy with cannabis-based medications. For adult patients with ADHD, who experience side effects or do not profit from standard medication, cannabis may be an effective and well-tolerated alternative. Treating Adult ADHD with Cannabis Cancer PDf
The approval of this Petition: Requesting The Inclusion Of A New Medical Condition(s): ADD/ADHD, Anxiety, And Tourette's Syndrome, that is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
The approval of this petition would bring the Department of Health in compliance with the intent of the law and uphold the spirit of the Lynn and Erin Compassionate Use Act, 2007. Fulfilling both;
- Six weeks of cannabis treatment reduced tics in patients with Tourette’s with no serious adverse effects or impairment on neuropsychological performance. Cannabinoids reduce symptoms of Tourette’s syndrome.(http://www.tandfonline.com/doi/pdf/10.1517/14656566.4.10.1717?needAccess=true)
- A significant reduction in tics was seen in Tourette’s syndrome patients after six weeks of cannabis treatment. Delta 9-tetrahydrocannabinol (THC) is effective in the treatment of tics in Tourette syndrome: a 6-week randomized trial.(http://www.psychiatrist.com/jcp/article/Pages/2003/v64n04/v64n0417.aspx)
A new 2017 study indeed demonstrates the efficacy of an oral mucosal cannabinoid drug, Sativex, in a small sample of 30 adults diagnosed with ADHD (Cooper et al., 2017). Collectively, these findings begin to define a complex relationship between cannabis use and patients with ADHD, as well as its implications on cannabis/cannabinoids as a potential treatment for patients with this disorder. This article will examine the data from this study while also exploring other relevant and available data surrounding the potential use of cannabis in the treatment of ADHD.
One conditioning gaining popularity as a viable candidate for cannabinoid therapy is Attention Deficit Hyperactivity Disorder (ADHD). A new 2017 study performed by Cooper and colleagues piloted a randomized, placebo-controlled study involving the administration of Sativex, a whole plant cannabinoid medication, to 20 adults diagnosed with ADHD (Cooper et al., 2017). While the results of this study suggest the benefits of cannabis in the treatment of ADHD may be largely subjective, emerging data seems to suggest that the endocannabinoid system may be implicated in the pathophysiology of ADHD and should therefore be further investigated.
The mechanism for cannabinoids in the pathology of ADHD is still largely unknown, however, it is thought to be related to enhanced dopaminergic transmission (Cooper et al., 2017). This enhanced dopamine activity is the reason stimulants are considered the “gold standard” for pharmacotreatment of ADHD (Punja et al., 2016). Physicians, however, are sometimes reluctant to prescribe such psychotropic drugs to a population of patients commonly presenting with a comorbidity for substance abuse.
The same reluctance may be a factor in using cannabis, a widely abused drug, in the treatment of ADHD as well. However, this author argues that the side effect profile of cannabis may be better tolerated than that of stimulants. Insomnia is one of the most commonly reported side effects of stimulant medication and can have significantly detrimental effects on the patient, especially in children (Punja et al., 2016).
A 12-year comprehensive review showed a steep rise in stimulant medications (0.6% in 1987 to 2.7% in 1997) prescribed to children over time for the treatment of ADHD (Zuvekas & Vitiello, 2012). The use of these powerful psychotropic meds in children has begun to spur some controversy. A similar concern presents itself when considering cannabis treatment for ADHD in pediatric patients. More research is beginning to emerge on the role of cannabis in the developing brain and the results warrant further investigation into cannabis therapy in pediatric patients.
In trying to understand the role of cannabis use in the developing brain, it is critical to explore the documented neurocognitive effects of cannabis in children and adolescents. Recent attention has been brought to remarkably dramatic case reports of children with debilitating illnesses failing to respond to traditional medicine and for whom cannabis is the only solution. As such, there are an increasing number of pediatric and adolescent patients being added to the medical cannabis registry, particularly for conditions such as epilepsy (Handland et al., 2016).
According to highly specialized medical cannabis doctor Dr. Bonni Goldstein, ”There are many patients who suffer with Tourette syndrome (TS) who are finding relief of symptoms with cannabis.” Goldstein further added, “A large percentage of people who have been diagnosed with TS also suffer with other significant conditions, such as OCD, ADHD, mood disorders and anxiety. The conventional medications used to treat these conditions are not always helpful and often cause a wide array of unwanted side effects.”
Treating Adult ADHD with Cannabis
The Society of Cannabis Clinicians also states that; The medical certificates of 30 patients with adult ADHD, who were granted approval by the German Health Ministry to use cannabis flowers between 2012 and 2014, were analysed with regard to course of disease, previous treatment efforts, and effects of self-medication with cannabis or therapy with cannabis-based medications. For adult patients with ADHD, who experience side effects or do not profit from standard medication, cannabis may be an effective and well-tolerated alternative. Treating Adult ADHD with Cannabis Cancer PDf
Rules, Regulations, & Policy Solution For This Petition: Requesting The Inclusion Of A New Medical Condition(s): ADD/ADHD, Anxiety, And Tourette's Syndrome
The approval of this petition would bring the Department of Health in compliance with the intent of the law and uphold the spirit of the Lynn and Erin Compassionate Use Act, 2007. Fulfilling both;
“Section 2. PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments”
And Section 6. ADVISORY BOARD CREATED--DUTIES: The advisory board shall: A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis.”
New Mexico’s medical cannabis history started in 1978. After public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis...the first law.
Adults with ADHD are likely to have an anxiety disorder, depression, bipolar disorder, or other comorbid psychiatric disorder. (The term “comorbid” refers to a condition that exists with another.) About 50 percent of adults with ADHD also suffer from an anxiety disorder.
[https://adaa.org/understanding-anxiety/related-illnesses/other-related-conditions/adult-adhd]
1. The Potential of Cannabinoid-Based Treatments in Tourette Syndrome.
Novel pharmacological treatments are needed for Tourette syndrome. Our goal was to examine the current evidence base and biological rationale for the use of cannabis-derived medications or medications that act on the cannabinoid system in Tourette syndrome. We conducted a comprehensive literature search of PubMed for randomized controlled trials or clinical trials of cannabis-derived medications in Tourette syndrome. Data regarding the population, intervention, safety profile, and outcomes for each trial were extracted and reported and the evidence supporting use of individual cannabis-derived medications was critiqued. There is a strong biological rationale regarding how cannabis-derived medications could affect tic severity. Anecdotal case reports and series have noted that many patients report that their tics improve after using cannabis. However, only two small randomized, placebo-controlled trials of Δ9-tetrahydrocannabinol have been published; these suggested possible benefits of cannabis-derived agents for the treatment of tics. Trials examining other agents active on the cannabinoid system for tic disorders are currently ongoing. Cannabinoid-based treatments are a promising avenue of new research for medications that may help the Tourette syndrome population. However, given the limited research available, the overall efficacy and safety of cannabinoid-based treatments is largely unknown. Further trials are needed to examine dosing, active ingredients, and optimal mode of administration of cannabis-derived compounds, assuming initial trials suggest efficacy. Clinical use for refractory patients should at the very least be restricted to adult populations, given the uncertain efficacy and risk of developmental adverse effects that cannabinoids may have in children. Even in adult populations, cannabis-derived medications are associated with significant issues such as the effects they have on driving safety and the fact that they cause positive urine drug screens that can affect employment.
[https://link.springer.com/article/10.1007%2Fs40263-019-00627-1]
2. “I Use Weed for My ADHD”: A Qualitative Analysis of Online Forum Discussions on Cannabis Use and ADHD
Abstract
Background
Attention-deficit/hyperactivity disorder (ADHD) is a risk factor for problematic cannabis use. However, clinical and anecdotal evidence suggest an increasingly popular perception that cannabis is therapeutic for ADHD, including via online resources. Given that the Internet is increasingly utilized as a source of healthcare information and may influence perceptions, we conducted a qualitative analysis of online forum discussions, also referred to as threads, on the effects of cannabis on ADHD to systematically characterize the content patients and caregivers may encounter about ADHD and cannabis.
Methods
A total of 268 separate forum threads were identified. Twenty percent (20%) were randomly selected, which yielded 55 separate forum threads (mean number of individual posts per forum thread = 17.53) scored by three raters (Cohen’s kappa = 0.74). A final sample of 401 posts in these forum threads received at least one endorsement on predetermined topics following qualitative coding procedures.
Results
Twenty-five (25%) percent of individual posts indicated that cannabis is therapeutic for ADHD, as opposed to 8% that it is harmful, 5% that it is both therapeutic and harmful, and 2% that it has no effect on ADHD. This pattern was generally consistent when the year of each post was considered. The greater endorsement of therapeutic versus harmful effects of cannabis did not generalize to mood, other (non-ADHD) psychiatric conditions, or overall domains of daily life. Additional themes emerged (e.g., cannabis being considered sanctioned by healthcare providers).
Conclusions
Despite that there are no clinical recommendations or systematic research supporting the beneficial effects of cannabis use for ADHD, online discussions indicate that cannabis is considered therapeutic for ADHD—this is the first study to identify such a trend. This type of online information could shape ADHD patient and caregiver perceptions, and influence cannabis use and clinical care.
[https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0156614]
3. Reduction of Benzodiazepine Use in Patients Prescribed Medical Cannabis
Abstract
Background: Benzodiazepines are a class of medication with sedative properties, commonly used for anxiety and other neurological conditions. These medications are associated with several well-known adverse effects. This observational study aims to investigate the reduction of benzodiazepine use in patients using prescribed medical cannabis.
Methods: A retrospective analysis was performed on a cohort of 146 medical cannabis patients (average age 47 years, 61% female, 54% reporting prior use of cannabis) who reported benzodiazepine use at initiation of cannabis therapy. These data are a part of a database gathered by a medical cannabis clinic (Canabo Medical). Descriptive statistics were used to quantify associations of the proportion of benzodiazepine use with time on medical cannabis therapy.
Results: After completing an average 2-month prescription course of medical cannabis, 30.1% of patients had discontinued benzodiazepines. At a follow-up after two prescriptions, 65 total patients (44.5%) had discontinued benzodiazepines. At the final follow-up period after three medical cannabis prescription courses, 66 total patients (45.2%) had discontinued benzodiazepine use, showing a stable cessation rate over an average of 6 months.
Conclusion: Within a cohort of 146 patients initiated on medical cannabis therapy, 45.2% patients successfully discontinued their pre-existing benzodiazepine therapy. This observation merits further investigation into the risks and benefits of the therapeutic use of medical cannabis and its role relating to benzodiazepine use.
Narrative:
Researchers discovered that nearly half of patients discontinued their use of anti-anxiety meds after starting with medical cannabis.
Findings in a new study published in Cannabis and Cannabinoid Research suggest that cannabis can be used as an effective alternative to traditional anti-anxiety medications.
A team of Canadian researchers assessed the relationship between cannabis and benzodiazepines, a class of drugs that work in the central nervous system and are primarily used for treating anxiety. Common benzodiazepines include Xanax, Ativan, and Valium.
Using a cohort of 146 patients enrolled in Canada’s medical marijuana program, the researchers discovered a large portion of patients had substituted cannabis for their anti-anxiety drugs.
Specifically, the cannabis in place of benzodiazepines study found that 30 percent of patients reported discontinuing their use of benzodiazepines within two months of starting medical cannabis treatment. By the six-month check-in with their cannabis doctor, 45 percent of patients stopped anti-anxiety medication use.
The participating patients, once initiating medical marijuana use, also reported decreased daily distress from their medical conditions.
While doctors commonly prescribe benzodiazepines to treating anxiety, the drugs also associated with potentially serious side effects and risks. According to the United States Centers for Disease Control and Prevention, the drug was attributed to over 11,500 fatal overdoses in 2017. Nobody has ever reportedly died of a cannabis overdose.
“The study results are encouraging, and this work is concurrent with growing public interest in a rapidly developing Canadian cannabis market,” said lead author of the cannabis in place of benzodiazepines study, Chad Purcell.
“We are advising the public to observe caution. The results do not suggest that cannabis should be used as an alternative to conventional therapies. Our purpose is inspiring others to advance current cannabis understanding as we collect stronger efficacy and safety data that will lead to responsible policy and recommended practices for use.”
The new cannabis in place of benzodiazepines study, “Reduction of Benzodiazepine Use in Patients Prescribed Medical Cannabis,” is available to access in full for free through the journal Cannabis and Cannabinoid Research.
[https://www.liebertpub.com/doi/full/10.1089/can.2018.0020]
4. Differential Regulation of the Endocannabinoids Anandamide and 2-Arachidonylglycerol within the Limbic Forebrain by Dopamine Receptor Activity
Sachin Patel, David J. Rademacher and Cecilia J. Hillard
Journal of Pharmacology and Experimental Therapeutics September 2003, 306 (3) 880-888; DOI: https://doi.org/10.1124/jpet.103.054270
[http://jpet.aspetjournals.org/content/306/3/880.full]
5. S.12.08 - Cannabinoids in attention-deficit/hyperactivity disorder: a randomised-controlled trial
R.E.CooperE.WilliamsS.SeegobinC.TyeJ.KuntsiP.Asherson
[https://www.sciencedirect.com/science/article/abs/pii/S0924977X16309129]
6. Cannabis improves symptoms of ADHD
Peter Strohbeck-Kuehner, Gisela Skopp, Rainer Mattern Institute of Legal- and Traffic Medicine, Heidelberg University Medical Centre, Voss Str. 2, D-69115 Heidelberg, Germany
Abstract: Attention-deficit/hyperactivity disorder (ADHD) is characterized by attention deficits and an altered activation level. The purpose of this case investigation was to highlight that people with ADHD can benefit in some cases from the consumption of THC. A 28-year old male, who showed improper behaviour and appeared to be very maladjusted and inattentive while sober, appeared to be completely inconspicuous while having a very high blood plasma level of delta-9- tetrahydrocannabinol (THC). Performance tests, which were conducted with the test batteries ART2020 and TAP provided sufficient and partly over-averaged results in driving related performance. Thus, it has to be considered, that in the case of ADHD, THC can have atypical effects and can even lead to an enhanced driving related performance. Keywords: ADHD, cannabis, performance, driving
[http://cannabis-med.org/data/pdf/en_2008_01_1.pdf]
7. Scientists at Washington State University published a study in the Journal of Affective Disorders that found that smoking cannabis can significantly reduce self-reported levels of depression, anxiety, and stress in the short term.
Highlights
Background
Cannabis is commonly used to alleviate symptoms of negative affect. However, a paucity of research has examined the acute effects of cannabis on negative affect in everyday life. The current study provides a naturalistic account of perceived changes in symptoms of depression, anxiety, and stress as a function of dose and concentration of Δ9tetrahydrocannabinol (THC) and cannabidiol (CBD).
Method
Data from the app StrainprintTM (which provides medical cannabis users a means of tracking changes in symptoms as a function of different doses and chemotypes of cannabis) were analyzed using multilevel modeling. In total, 11,953 tracked sessions were analyzed (3,151 for depression, 5,085 for anxiety, and 3,717 for stress).
Results
Medical cannabis users perceived a 50% reduction in depression and a 58% reduction in anxiety and stress following cannabis use. Two puffs were sufficient to reduce ratings of depression and anxiety, while 10+ puffs produced the greatest perceived reductions in stress. High CBD (>9.5%)/low THC (<5.5%) cannabis was associated with the largest changes in depression ratings, while high CBD (>11%)/high THC (>26.5%) cannabis produced the largest perceived changes in stress. No changes in the perceived efficacy of cannabis were detected across time. However, baseline symptoms of depression (but not anxiety or stress) appeared to be exacerbated across time/tracked sessions.
[https://www.sciencedirect.com/science/article/pii/S0165032718303100?via%3Dihub]
8. Patient-reported use of medical cannabis for pain, anxiety, and depression symptoms: Systematic review and meta-analysis
Highlights
Rationale
Certifications for medical cannabis are generally restricted to a small number of specific medical conditions, yet patients frequently report symptoms of pain, anxiety, and depression as reasons for use. This is a critical concern for researchers, healthcare providers, and policymakers, yet research in this area is currently obstructed by the lack of a focused review or empirical synthesis on patient-reported reasons for medical cannabis use.
Objectives
AND METHOD: The first aim of this project was to conduct the first systematic review and meta-analysis of empirical studies of patient-reported symptoms of pain, anxiety, and depression as reasons for medical cannabis use. The second aim was to conduct an empirical assessment of the methodological quality of extant research, test for publication bias, and test sex composition and quality scores of individual studies as possible sources of observed heterogeneity.
Results
Meta-analytic results indicated that pain (64%), anxiety (50%), and depression/mood (34%) were common reasons for medical cannabis use. No evidence for publication bias was detected, despite heterogeneity in prevalence rates. A comprehensive assessment of study quality identified a number of specific methodological limitations of the existing research, including challenges in patient recruitment, use of restrictive sampling frames, and a lack of randomized recruitment methods and validated assessment measures.
Conclusion
Findings are discussed with regard to possible explanations for current results, clinical considerations, and areas of future research that are needed to move the field forward.
[https://www.sciencedirect.com/science/article/abs/pii/S0277953619303272]
9. Currently ADD/ADHD is a qualifying health condition in these state comprehensive medical cannabis program; California, Washington DC, Guam, Massachusetts, Maine, Maryland, Missouri, and Oklahoma.
Currently Anxiety is a qualifying health condition in these state comprehensive medical cannabis program; California, Washington DC, Guam, Massachusetts, Maine, Maryland, Missouri, North Dakota, New Jersey, Oklahoma, Pennsylvania, Puerto Rico, Virginia, and Wisconsin.
Currently Tourette’s is a qualifying health condition in these state comprehensive medical cannabis program; Arkansas, California, Connecticut, Washington DC, Guam, Illinois, Massachusetts, Maine, Maryland, Minnesota, New Hampshire, Ohio, Oklahoma, Pennsylvania, Virginia, and Wisconsin.
State and Territory Qualifying Condition Chart (The chart is current as of August 12, 2019.)
New Research Added to Petition for the December 10th MCAB Hearing:
[https://adaa.org/understanding-anxiety/related-illnesses/other-related-conditions/adult-adhd]
1. The Potential of Cannabinoid-Based Treatments in Tourette Syndrome.
Novel pharmacological treatments are needed for Tourette syndrome. Our goal was to examine the current evidence base and biological rationale for the use of cannabis-derived medications or medications that act on the cannabinoid system in Tourette syndrome. We conducted a comprehensive literature search of PubMed for randomized controlled trials or clinical trials of cannabis-derived medications in Tourette syndrome. Data regarding the population, intervention, safety profile, and outcomes for each trial were extracted and reported and the evidence supporting use of individual cannabis-derived medications was critiqued. There is a strong biological rationale regarding how cannabis-derived medications could affect tic severity. Anecdotal case reports and series have noted that many patients report that their tics improve after using cannabis. However, only two small randomized, placebo-controlled trials of Δ9-tetrahydrocannabinol have been published; these suggested possible benefits of cannabis-derived agents for the treatment of tics. Trials examining other agents active on the cannabinoid system for tic disorders are currently ongoing. Cannabinoid-based treatments are a promising avenue of new research for medications that may help the Tourette syndrome population. However, given the limited research available, the overall efficacy and safety of cannabinoid-based treatments is largely unknown. Further trials are needed to examine dosing, active ingredients, and optimal mode of administration of cannabis-derived compounds, assuming initial trials suggest efficacy. Clinical use for refractory patients should at the very least be restricted to adult populations, given the uncertain efficacy and risk of developmental adverse effects that cannabinoids may have in children. Even in adult populations, cannabis-derived medications are associated with significant issues such as the effects they have on driving safety and the fact that they cause positive urine drug screens that can affect employment.
[https://link.springer.com/article/10.1007%2Fs40263-019-00627-1]
2. “I Use Weed for My ADHD”: A Qualitative Analysis of Online Forum Discussions on Cannabis Use and ADHD
Abstract
Background
Attention-deficit/hyperactivity disorder (ADHD) is a risk factor for problematic cannabis use. However, clinical and anecdotal evidence suggest an increasingly popular perception that cannabis is therapeutic for ADHD, including via online resources. Given that the Internet is increasingly utilized as a source of healthcare information and may influence perceptions, we conducted a qualitative analysis of online forum discussions, also referred to as threads, on the effects of cannabis on ADHD to systematically characterize the content patients and caregivers may encounter about ADHD and cannabis.
Methods
A total of 268 separate forum threads were identified. Twenty percent (20%) were randomly selected, which yielded 55 separate forum threads (mean number of individual posts per forum thread = 17.53) scored by three raters (Cohen’s kappa = 0.74). A final sample of 401 posts in these forum threads received at least one endorsement on predetermined topics following qualitative coding procedures.
Results
Twenty-five (25%) percent of individual posts indicated that cannabis is therapeutic for ADHD, as opposed to 8% that it is harmful, 5% that it is both therapeutic and harmful, and 2% that it has no effect on ADHD. This pattern was generally consistent when the year of each post was considered. The greater endorsement of therapeutic versus harmful effects of cannabis did not generalize to mood, other (non-ADHD) psychiatric conditions, or overall domains of daily life. Additional themes emerged (e.g., cannabis being considered sanctioned by healthcare providers).
Conclusions
Despite that there are no clinical recommendations or systematic research supporting the beneficial effects of cannabis use for ADHD, online discussions indicate that cannabis is considered therapeutic for ADHD—this is the first study to identify such a trend. This type of online information could shape ADHD patient and caregiver perceptions, and influence cannabis use and clinical care.
[https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0156614]
3. Reduction of Benzodiazepine Use in Patients Prescribed Medical Cannabis
Abstract
Background: Benzodiazepines are a class of medication with sedative properties, commonly used for anxiety and other neurological conditions. These medications are associated with several well-known adverse effects. This observational study aims to investigate the reduction of benzodiazepine use in patients using prescribed medical cannabis.
Methods: A retrospective analysis was performed on a cohort of 146 medical cannabis patients (average age 47 years, 61% female, 54% reporting prior use of cannabis) who reported benzodiazepine use at initiation of cannabis therapy. These data are a part of a database gathered by a medical cannabis clinic (Canabo Medical). Descriptive statistics were used to quantify associations of the proportion of benzodiazepine use with time on medical cannabis therapy.
Results: After completing an average 2-month prescription course of medical cannabis, 30.1% of patients had discontinued benzodiazepines. At a follow-up after two prescriptions, 65 total patients (44.5%) had discontinued benzodiazepines. At the final follow-up period after three medical cannabis prescription courses, 66 total patients (45.2%) had discontinued benzodiazepine use, showing a stable cessation rate over an average of 6 months.
Conclusion: Within a cohort of 146 patients initiated on medical cannabis therapy, 45.2% patients successfully discontinued their pre-existing benzodiazepine therapy. This observation merits further investigation into the risks and benefits of the therapeutic use of medical cannabis and its role relating to benzodiazepine use.
Narrative:
Researchers discovered that nearly half of patients discontinued their use of anti-anxiety meds after starting with medical cannabis.
Findings in a new study published in Cannabis and Cannabinoid Research suggest that cannabis can be used as an effective alternative to traditional anti-anxiety medications.
A team of Canadian researchers assessed the relationship between cannabis and benzodiazepines, a class of drugs that work in the central nervous system and are primarily used for treating anxiety. Common benzodiazepines include Xanax, Ativan, and Valium.
Using a cohort of 146 patients enrolled in Canada’s medical marijuana program, the researchers discovered a large portion of patients had substituted cannabis for their anti-anxiety drugs.
“Patients initiated on medical cannabis therapy showed significant benzodiazepine discontinuation rates after their first follow-up visit to their medical cannabis provider, and continued to show discontinuation rates thereafter,” the study concluded.
Specifically, the cannabis in place of benzodiazepines study found that 30 percent of patients reported discontinuing their use of benzodiazepines within two months of starting medical cannabis treatment. By the six-month check-in with their cannabis doctor, 45 percent of patients stopped anti-anxiety medication use.
The participating patients, once initiating medical marijuana use, also reported decreased daily distress from their medical conditions.
While doctors commonly prescribe benzodiazepines to treating anxiety, the drugs also associated with potentially serious side effects and risks. According to the United States Centers for Disease Control and Prevention, the drug was attributed to over 11,500 fatal overdoses in 2017. Nobody has ever reportedly died of a cannabis overdose.
“The study results are encouraging, and this work is concurrent with growing public interest in a rapidly developing Canadian cannabis market,” said lead author of the cannabis in place of benzodiazepines study, Chad Purcell.
“We are advising the public to observe caution. The results do not suggest that cannabis should be used as an alternative to conventional therapies. Our purpose is inspiring others to advance current cannabis understanding as we collect stronger efficacy and safety data that will lead to responsible policy and recommended practices for use.”
The new cannabis in place of benzodiazepines study, “Reduction of Benzodiazepine Use in Patients Prescribed Medical Cannabis,” is available to access in full for free through the journal Cannabis and Cannabinoid Research.
[https://www.liebertpub.com/doi/full/10.1089/can.2018.0020]
4. Differential Regulation of the Endocannabinoids Anandamide and 2-Arachidonylglycerol within the Limbic Forebrain by Dopamine Receptor Activity
Sachin Patel, David J. Rademacher and Cecilia J. Hillard
Journal of Pharmacology and Experimental Therapeutics September 2003, 306 (3) 880-888; DOI: https://doi.org/10.1124/jpet.103.054270
[http://jpet.aspetjournals.org/content/306/3/880.full]
5. S.12.08 - Cannabinoids in attention-deficit/hyperactivity disorder: a randomised-controlled trial
R.E.CooperE.WilliamsS.SeegobinC.TyeJ.KuntsiP.Asherson
[https://www.sciencedirect.com/science/article/abs/pii/S0924977X16309129]
6. Cannabis improves symptoms of ADHD
Peter Strohbeck-Kuehner, Gisela Skopp, Rainer Mattern Institute of Legal- and Traffic Medicine, Heidelberg University Medical Centre, Voss Str. 2, D-69115 Heidelberg, Germany
Abstract: Attention-deficit/hyperactivity disorder (ADHD) is characterized by attention deficits and an altered activation level. The purpose of this case investigation was to highlight that people with ADHD can benefit in some cases from the consumption of THC. A 28-year old male, who showed improper behaviour and appeared to be very maladjusted and inattentive while sober, appeared to be completely inconspicuous while having a very high blood plasma level of delta-9- tetrahydrocannabinol (THC). Performance tests, which were conducted with the test batteries ART2020 and TAP provided sufficient and partly over-averaged results in driving related performance. Thus, it has to be considered, that in the case of ADHD, THC can have atypical effects and can even lead to an enhanced driving related performance. Keywords: ADHD, cannabis, performance, driving
[http://cannabis-med.org/data/pdf/en_2008_01_1.pdf]
7. Scientists at Washington State University published a study in the Journal of Affective Disorders that found that smoking cannabis can significantly reduce self-reported levels of depression, anxiety, and stress in the short term.
Highlights
- Cannabis significantly reduced ratings of depression, anxiety, and stress.
- Women reported larger reductions in anxiety as a function of cannabis than did men.
- Low THC/high CBD cannabis was best for reducing perceived symptoms of depression.
- High THC/high CBD cannabis was best for reducing perceived symptoms of stress.
- Use of cannabis to treat depression appears to exacerbate depression over time.
Background
Cannabis is commonly used to alleviate symptoms of negative affect. However, a paucity of research has examined the acute effects of cannabis on negative affect in everyday life. The current study provides a naturalistic account of perceived changes in symptoms of depression, anxiety, and stress as a function of dose and concentration of Δ9tetrahydrocannabinol (THC) and cannabidiol (CBD).
Method
Data from the app StrainprintTM (which provides medical cannabis users a means of tracking changes in symptoms as a function of different doses and chemotypes of cannabis) were analyzed using multilevel modeling. In total, 11,953 tracked sessions were analyzed (3,151 for depression, 5,085 for anxiety, and 3,717 for stress).
Results
Medical cannabis users perceived a 50% reduction in depression and a 58% reduction in anxiety and stress following cannabis use. Two puffs were sufficient to reduce ratings of depression and anxiety, while 10+ puffs produced the greatest perceived reductions in stress. High CBD (>9.5%)/low THC (<5.5%) cannabis was associated with the largest changes in depression ratings, while high CBD (>11%)/high THC (>26.5%) cannabis produced the largest perceived changes in stress. No changes in the perceived efficacy of cannabis were detected across time. However, baseline symptoms of depression (but not anxiety or stress) appeared to be exacerbated across time/tracked sessions.
[https://www.sciencedirect.com/science/article/pii/S0165032718303100?via%3Dihub]
8. Patient-reported use of medical cannabis for pain, anxiety, and depression symptoms: Systematic review and meta-analysis
Highlights
- Systematically reviewed studies why patients use medical cannabis.
- Pain was a common reason for medical cannabis use (64%).
- Anxiety (50%) and depression (34%) were also common reasons for use.
- Prevalence rates were heterogeneous; no apparent publication bias.
- Review offers specific directions for future research.
Rationale
Certifications for medical cannabis are generally restricted to a small number of specific medical conditions, yet patients frequently report symptoms of pain, anxiety, and depression as reasons for use. This is a critical concern for researchers, healthcare providers, and policymakers, yet research in this area is currently obstructed by the lack of a focused review or empirical synthesis on patient-reported reasons for medical cannabis use.
Objectives
AND METHOD: The first aim of this project was to conduct the first systematic review and meta-analysis of empirical studies of patient-reported symptoms of pain, anxiety, and depression as reasons for medical cannabis use. The second aim was to conduct an empirical assessment of the methodological quality of extant research, test for publication bias, and test sex composition and quality scores of individual studies as possible sources of observed heterogeneity.
Results
Meta-analytic results indicated that pain (64%), anxiety (50%), and depression/mood (34%) were common reasons for medical cannabis use. No evidence for publication bias was detected, despite heterogeneity in prevalence rates. A comprehensive assessment of study quality identified a number of specific methodological limitations of the existing research, including challenges in patient recruitment, use of restrictive sampling frames, and a lack of randomized recruitment methods and validated assessment measures.
Conclusion
Findings are discussed with regard to possible explanations for current results, clinical considerations, and areas of future research that are needed to move the field forward.
[https://www.sciencedirect.com/science/article/abs/pii/S0277953619303272]
9. Currently ADD/ADHD is a qualifying health condition in these state comprehensive medical cannabis program; California, Washington DC, Guam, Massachusetts, Maine, Maryland, Missouri, and Oklahoma.
Currently Anxiety is a qualifying health condition in these state comprehensive medical cannabis program; California, Washington DC, Guam, Massachusetts, Maine, Maryland, Missouri, North Dakota, New Jersey, Oklahoma, Pennsylvania, Puerto Rico, Virginia, and Wisconsin.
Currently Tourette’s is a qualifying health condition in these state comprehensive medical cannabis program; Arkansas, California, Connecticut, Washington DC, Guam, Illinois, Massachusetts, Maine, Maryland, Minnesota, New Hampshire, Ohio, Oklahoma, Pennsylvania, Virginia, and Wisconsin.
State and Territory Qualifying Condition Chart (The chart is current as of August 12, 2019.)
 |
| Credit: ASA |
Link: https://onedrive.live.com/View.aspx?resid=AC37A4F52EDA656A!136&authkey=!AEvQ5uaj2Lo1E5g
Link to Chart Key: https://www.safeaccessnow.org/condition
Additional References:
Abi-Jaoude, E., Chen, L., Cheung, P., Bhikram, T., and Sandor, P. (2017, May 3). Preliminary evidence on cannabis effectiveness and tolerability for adults with Tourette syndrome. The Journal of Neuropsychiatry and Clinical Neurosciences, appineuropsych 16110310. doi: 10.1176/appi.neuropsych.16110310. [Epub ahead of print]. Retrieved from http://neuro.psychiatryonline.org/doi/full/10.1176/appi.neuropsych.16110310.
Curtis, A., Clarke, C.E., and Rickards, H.E. (2009, October 7). Cannabinoids for Tourette’s Syndrome (Review). The Cochrane Database of Systematic Reviews, (4), CD006565, doi: 10.1002/14651858.pub2. Retrieved from http://onlinelibrary.wiley.com/wol1/doi/10.1002/14651858.CD006565.pub2/full.
Facts About Tourette Syndrome. (2015, June 10). Centers for Disease Control and Prevention. Retrieved from http://www.cdc.gov/ncbddd/tourette/facts.html.
Muller-Vahl, K.R., Kolbe, H., Schneider, U., and Emrich, H.M. (1998, December). Cannabinoids: possible role in patho-physiology and therapy of Gilles de la Tourette syndrome. Acta Psychiatra Scandinavica, 98(6), 502-6. Retrieved from http://onlinelibrary.wiley.com/doi/10.1111/j.1600-0447.1998.tb10127.x/pdf.
Muller-Vahl, K.R. (2003, October). Cannabinoids reduce symptoms of Tourette’s syndrome. Expert Opinion on Pharmacology, 4(10), 1717-25. Retrieved from http://www.tandfonline.com/doi/pdf/10.1517/14656566.4.10.1717?needAccess=true.
Muller-Vahl, K.R. (2013). Treatment of Tourette syndrome with cannabinoids. Behavioral Neurology, 27(1), 119-24. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5215298/.
Muller-Vahl, K.R., Koblenz, A., Jobges, M., Kolbe, H., Emrich, H.M., and Schneider, U. (2001, January). Influence of treatment of Tourette syndrome with delta9-tetrahydrocannabinol (delta9-THC) on neuropsychological performance. Pharmacopsychiatry, 34(1), 19-24. Retrieved from https://www.thieme-connect.com/DOI/DOI?10.1055/s-2001-15191.
Muller-Vahl, K.R., Prevedel, H., Theloe, K., Kolbe, H., Emrich, H.M., and Schneider, U. (2003, February). Treatment of Tourette syndrome with delta-9-tetrahydrocannabinol (delta 9-THC): no influence on neuropsychological performance. Neuropsychopharmacology, 28(2), 384-8. Retrieved from http://www.nature.com/npp/journal/v28/n2/full/1300047a.html.
Muller-Vahl, K.R., Schneider, U., Koblenz, A., Jobges, M., Kolbe, H., Daldrup, T., and Emrich, H.M. (2002, March). Treatment of Tourette’s syndrome with Delta 9-tetrahydrocannabinol (THC): a randomized crossover trial. Pharmacopsychiatry, 35(2), 57-61. Retrieved from https://www.thieme-connect.com/DOI/DOI?10.1055/s-2002-25028.
Muller-Vahl, K.R., Schneider, U., Prevedel, H., Theloe, K., Kolbe, H., Daldrup, T., and Emrich, H.M. (2003, April). Delta 9-tetrahydrocannabinol (THC) is effective in the treatment of tics in Tourette syndrome: a 6-week randomized trial. The Journal of Clinical Psychiatry, 64(4), 459-65. Retrieved from http://www.psychiatrist.com/jcp/article/Pages/2003/v64n04/v64n0417.aspx.
Tourette syndrome. (2012, August 10). Mayo Clinic. Retrieved from http://www.mayoclinic.org/diseases-conditions/tourette-syndrome/basics/definition/con-20043570.

No comments:
Post a Comment