

SafeAccessNewMexico@gmail.com
www.cannabisnewsjournal.co
Tuesday, April 10th 2018
New Mexico Department of Health
Medical Cannabis Advisory Board
Medical Cannabis Program
1474 Rodeo Rd., Suite 200
Santa Fe, NM 87505
Petition:
Requesting The Inclusion Of A New Medical Condition:
Autism Spectrum Disorders
Table of Contents
Pg. 1 Cover Page
Pg. 2 - 3 Petition Introduction
Pg. 3 Petition Purpose and Background
Pg. 4 - 16 Minnesota health department’s autism research brief
Pg. 17 - 18 Dr. Dustin Sulak (Integr8 Health) Interview
Pg. 19 - Petition Research Continued About Medical Cannabis and ASD
Pg. 22 - 31 Research Part One: Endocannabinoid System & Autism Spectrum Disorder
Pg. 31 - 36 Part Two: The Role of Phytocannabinoids in ASD Therapy
Pg. 37 - 41 Part Three: Practical Approach to Cannabis Based ASD Therapies
Pg. 41 Additional Research Showing How Medical Cannabis Benefits ASD
Pg. 42 Conclusion & Relief Requested In Petition
Pg. 43 End Page
Petition Introduction: Inclusion Of A New Medical Condition: Autism Spectrum Disorders
What is a chronic medical condition?
A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear. Harvard Medical Dictionary defines chronic as: Any condition that lasts a long time or recurs over time; chronic pain as: Pain that persists after an injury has healed or a disease is over; and chronic pain syndrome as : Long-term, severe pain that doesn't spring from an injury or illness, that interferes with daily life, and is often accompanied by other problems, such as depression, irritability, and anxiety.
What is the meaning of debilitating?
Something that's debilitating seriously affects someone or something's strength or ability to carry on with regular activities, like a debilitating illness. Debilitating comes from the Latin word debilis, meaning "weak." That's why you'll often see the adjective used to describe illness, despite the negative reference.
Petition Purpose and Background
The purpose of this petition is; Inclusion Of A New Medical Condition: Autism Spectrum Disorders.
This petition for the Inclusion Of A New Medical Condition: Autism Spectrum Disorders is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
Who Should Qualify for Medical Cannabis Use?
According to Americans For Safe Access Policy Studies & Research:
Background: The most fundamental aspect of medical cannabis laws is the relationship between a patient and their physician. It is often only the physician and the patient that possess information about a patient’s health condition. However, many public officials and others who oppose medical cannabis laws often make assumptions about people’s health. The media have even fomented such inappropriate assumptions by naming a category of patients “Young Able Bodied Males,” condemning certain patients by visual assessment alone.
Findings: The health care information discussed between a patient and physician is considered private and protected under federal HIPAA laws. It is typically the purview of state medical boards to assess whether a physician has inappropriately recommended cannabis to someone who should not be qualified. Studies have shown in some medical cannabis states that the majority of patients suffer from chronic pain, an ailment that is not obviously detectable by another person. Nevertheless, police will often harass and arrest patients based on the assumption that someone is faking their illness.
Position: Medical professionals should have an unrestricted ability to recommend cannabis therapeutics and that should not be impacted by law enforcement’s perceptions.
Americans For Safe Access policy further states:
“Qualifying medical condition” shall mean any condition for which treatment with medical cannabis would be beneficial, as determined by a patient's qualified medical professional, including but not limited to cancer, glaucoma, positive status for human immunodeficiency virus, acquired immune deficiency syndrome (AIDS), hepatitis C, amyotrophic lateral sclerosis (ALS), Crohn’s disease, Parkinson’s disease, post-traumatic stress disorder, arthritis, chronic pain, neuropathic and other intractable chronic pain, and multiple sclerosis.
“Qualifying patient” shall mean a person who has a written recommendation from a qualified medical professional for the medical use of cannabis.
State of Minnesota Health Department Director Adds Autism Spectrum Disorders into Minnesota Medical Cannabis Program
‘Medical cannabis program to add autism and obstructive sleep apnea as qualifying conditions’
Minnesota Commissioner of Health Dr. Ed Ehlinger announced the decision to add autism spectrum disorders and obstructive sleep apnea as new qualifying conditions for the state’s medical cannabis program.
“Any policy decisions about cannabis are difficult due to the relative lack of published scientific evidence,” said Commissioner Ehlinger. “However, there is increasing evidence for potential benefits of medical cannabis for those with severe autism and obstructive sleep apnea.”
This year, as in years past, the Minnesota Department of Health used a formal petitioning process to solicit public input on potential qualifying conditions. Throughout June and July, Minnesotans were invited to submit petitions to add qualifying conditions. The process included public comments, a citizens’ review panel and a set of research summaries for each condition prepared by Minnesota Department of Health staff.
Autism spectrum disorder is characterized by sustained social impairments in communication and interactions, and repetitive behaviors, interests or activities. Patients certified for the program because of autism must meet the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders – 5th edition) for autism. The health department’s autism research brief (PDF) found a growing body of research indicating that the human body’s endocannabinoid system does play a role in autism symptoms. In support of adding autism, the review panel report (PDF) noted the lack of effective drug treatments, the potentially severe side effects of current drug treatments and anecdotal evidence of Minnesota children with autism already receiving benefits from medical cannabis taken for other qualifying conditions.
Minnesota health department’s autism research brief copy: Autism Spectrum Disorder(ASD)
ISSUE BRIEF ON AUTISM SPECTRUM DISORDER (ASD)
Introduction
Briefings such as this one are prepared in response to petitions to add new conditions to the list of qualifying conditions for the Minnesota medical cannabis program. The intention of these briefings is to present to the Commissioner of Health, to members of the Medical Cannabis Review Panel, and to interested members of the public scientific studies of cannabis products as therapy for the petitioned condition. Brief information on the condition and its current treatment is provided to help give context to the studies. The primary focus is on clinical trials and observational studies, but for many conditions there are few of these. A selection of articles on pre-clinical studies (typically laboratory and animal model studies) will be included, especially if there are few clinical trials or observational studies. Though interpretation of surveys is usually difficult because it is unclear whether responders represent the population of interest and because of unknown validity of responses, when published in peer-reviewed journals surveys will be included for completeness. When found, published recommendations or opinions of national organizations medical organizations will be included.
Searches for published clinical trials and observational studies of cannabis therapy are performed using the National Library of Medicine’s MEDLINE database using key words appropriate for the petitioned condition. Articles that appeared to be results of clinical trials, observational studies, or review articles of such studies, were accessed for examination. References in the articles were studied to identify additional articles that were not found on the initial search. This continued in an iterative fashion until no additional relevant articles were found. Finally, the federal government-maintained web site of clinical trials, clinicatrials.gov, was searched to learn about trials currently under way or under development and to check whether additional articles on completed trials could be found.
Definition
Autism spectrum disorder (ASD) is a neurodevelopmental disorder that is characterized by sustained social impairments in reciprocal social communication and interactions; and repetitive behaviors, interests, or activities. These essential markers of autism spectrum disorder present in early childhood and limit everyday functioning. The word “spectrum” is used to define ASD since the disorder manifests itself in diverse ways, depending on varying symptom severity, the individual’s development level, and chronological age (American Psychiatric Association 2013. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) is the 2013 update to the American Psychiatric Association’s classification and diagnostic tool. In the U.S. the DSM serves as the primary authority for psychiatric diagnosis. In the latest version of the DSM, several disorders have now been incorporated into the ASD definition, such as Kanner’s autism and Asperger’s disorder, among others. To be diagnosed with ASD, a person needs to fulfil the following criteria (American Psychiatric Association 2013):
Persistent deficits in social communication and interaction across multiple contexts, as demonstrated by all of the following:
- Deficits in social-emotional reciprocity, ranging, for example, from abnormal social approach and inability to have normal back-and-forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.
- Deficits in nonverbal communicative behaviors used for social interaction, ranging, for example, from poorly integrated verbal and nonverbal communication; to abnormalities in eye contact and body language or deficits in understanding and use of gestures; to a total lack of facial expressions and nonverbal communication.
- Deficits in developing, maintaining, and understanding relationships, ranging, for example, from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or in making friends; to absence of interest in peers.
Restricted, repetitive patterns of behavior, interests, or activities, as manifested by at least two of the following:
- Stereotyped or repetitive motor movements, use of objects, or speech (e.g., repetitive hand flapping, lining up toys or flipping objects, delayed or immediate parroting of others’ speech, idiosyncratic phrases).
- Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat same food every day).
- Highly restricted, fixated interests that are abnormal in intensity or focus (e.g., a child who is extremely attached to a spoon, an adult who spends hours rewriting specific phrases).
- Extremely exaggerated or dulled reactions to sensations or unusual interest in sensory aspects of the environment (e.g., apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement).
(These criteria can be currently occurring or have occurred in the patient’s past. Examples are illustrative, not exhaustive.)
Symptoms must be present in the early developmental period. Though, symptoms may not become fully apparent until social demands exceed limited capacities. Symptoms may also be masked by learned strategies in later life.
Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and autism spectrum disorder frequently co-occur. Social communication should be below what is expected for general developmental level, in order to make comorbid diagnoses of autism spectrum disorder and intellectual disability
Prevalence
The Centers for Disease Control and Prevention estimates that 1 out of every 68 children in the United States has autism spectrum disorder. ASD is roughly 4.5 times more common among boys than girls (Christensen 2016). Since 2006, the prevalence of childhood ASD has increased by 23%, becoming a major public-health concern. This increase in prevalence can be attributed to better screening and the DSM-5’s broader definition of ASD, among other issues (Harrington and Allen 2014).
Among both children and adults, roughly 3.5 million Americans live with autism spectrum disorder. Annually, costs associated with children who have ASD are $61 billion in the United States. Adults living with ASD cost the U.S. $196 billion per year (Buescher 2014).
Current Therapies
Several behavioral, educational, and pharmaceutical treatments are used to manage ASD. Pharmaceutical treatments mostly target comorbid health problems, which are common in children living with ASD (McPheeters 2011).
Behavioral and developmental interventions are the primary treatments for ASD (Ospina 2008). There is a great variety in the kinds of behavioral and developmental interventions, which are organized into smaller subcategories (Ospina 2008). For example, within the continuum of behavioral and developmental interventions, applied behavioral analysis (ABA) is designed to teach socially appropriate behaviors and to decrease challenging behaviors (Harrington 2014, Ospina 2008). Another kind of behavior and developmental intervention is social skills training (SST), which targets social deficits (White 2007).
ABA-based therapies have demonstrated positive effects on language, adaptive, cognitive, and educational outcomes (Hanley 2001, Lovaas 1987, Warren 2011). However, there is a lack of high-quality randomized controlled trials (Warren 2011). The studies that do evaluate behavioral and developmental interventions are methodologically weak, include few participants, and do not evaluate long-term effects of interventions (Ospina 2008). Therefore, the evidence to determine which behavioral interventions are most effective in children with ASD is inadequate (Warren et al., 2011). Studies on SST interventions are similarly low-quality, though evidence from several small, initial studies indicate that SST is potentially beneficial to children with ASD (White 2007).
Common comorbidities in children with ASD include intellectual disability, constipation, sleep disorders, anxiety, ADHD, and seizure disorders (Harrington and Allen, 2014; McPheeters 2011). Treating comorbid mental-health issues in children with ASD is more challenging than treating common medical problems, such as constipation and sleep problems (Harrington 2014). Antipsychotic medications, serotonin-reuptake inhibitors, and stimulants are among the pharmaceuticals used to treat mental-health comorbidities (McPheeters 2011). However, despite the fact that medications are used to treat many children with ASD, there is little evidence to indicate that these pharmaceuticals are effective (McPheeters 2011). Drugs that do demonstrate benefits for challenging or repetitive behaviors, are unfortunately associated with adverse effects, limiting their use to patients with severe impairments or risk of injury (McPheeters 2011).
Turning to adolescents and young adults with ASD, studies examining the effectiveness of behavioral, pharmaceutical, and other therapies in this population are poor-quality (Taylor 2012). There is a dramatic lack of evidence on the best way to treat adolescents and young adults who have ASD (Dove 2012, Taylor 2012).
Pre-Clinical Research
A September, 2017 review by Zamberletti et al (Zamberletti 2017) provides a good overview of the lines of evidence from animal studies suggesting the endocannabinoid system (ECS) plays a role in autism. Recently, at least three articles (Doenni 206, Servadio 2016, and Wei 2016) have reported on studies that manipulated the ECS in mouse models of autism.
Zamberletti E, Gabaglio M, Parolaro D. The endocannabinoid system and autism spectrum disorders: Insights from animals. Int J Mol Sci 2017;18(9). pii: E1916. doi: 10.3390/ijms18091916
This review provides evidence of involvement of the ECS in autism through modulation of autism-like behaviors and research suggesting possible mechanisms of action.
Genetic-based models:
Fragile X syndrome (FXS) is the most common known genetic cause of ASD. A mouse model of FXS has been developed: the Fmr1 knockout mouse. Fmr1 mice have been shown to have dysregulated endocannabinoid signaling. And studies that inhibited different enzymes that degrade endocannabinoids showed improvement in autism- consistent behaviors.
Inbreeding has produced a group of mouse strains used as a model for idiopathic (cause unknown) autism because the mice exhibit behaviors consistent with those seen in humans with ASD, but with no known gene mutation causing the behaviors. Prominent among these strains is the BTBR mouse model. Treatment to increase the level of one endocannabinoid (AEA) resulted in reduced ASD-like behavior.
Environmental-based models – environmental manipulations in rodents conducted using the same agents that have been correlated with human autism:
The valproic acid (VPA) rat model has been used extensively to evaluate the possible involvement of the endocannabinoid system in ASD. VPA is an anti-epileptic drug. Several studies have shown use of VPA during pregnancy may cause neural tube defects and cognitive impairment in children. In animal studies, offspring of rats administered VPA during pregnancy show lower social interaction, increased repetitive/sterotyped behaviors, early signs of neurodevelopment impairment, and abnormal responses to painful and non-painful stimuli. Studies have been done administering to rats exposed to VPA in utero substances that inhibit the breakdown of an endocannabinoid (AEA). Results showed decrease in the autism-model behaviors, with greater decrease seen in males.
Both viral and bacterial infections during pregnancy have been linked to an increased risk to develop ASD in the offspring. Injection of pregnant rodents with the substance, polyinosine:cytosine (LPS), which mimics the immune activation seen with the influenza virus, produces ASD-like behaviors in the offspring. These include impairments in social interaction and communication, stereotyped patterns of behavior, anxiety, and impaired learning and memory. These behaviors in the offspring were accompanied by distinctive changes in brain neuron structure and function. The tie to the endocannabinoid system comes with studies that administered LPS to rodents soon after birth. This resulted in decreased social play, reduced CB1 (cannabinoid receptor 1) binding, and increased levels of the endocannabinoid, AEA.
Possible mechanisms of action:
Studies have shown elements of the ECS interact with oxytocin, a neuropeptide that promotes parental and social bonding. Oxytocin stimulates endocannabinoid release in a relevant part of the brain (nucleus accumbens) and there is evidence endocannabinoid signaling is required for the prosocial effects of oxytocin.
mTOR signaling is involved in memory consolidation and normalization of mTOR signaling in the hippocampus reduces the cognitive deficits caused by cannabinoid receptor 1 blockade of Fmr1 (fragile X Syndrome model) mice. Dysregulation of mTOR signaling appears to be a feature common to a subset of ASD. (mTOR is an enzyme that controls cell growth and metabolism).
There is evidence that endocannabinoids might modulate ASD symptoms via interaction with immune system cells. Changes in endocannabinoid metabolism and in expression cannabinoid receptors (CB2) on certain white blood cells have been seen in ASD patients.
The authors conclude, “Although preclinical findings seem to suggest that pharmacological interventions aimed at modulating the EC system could be beneficial for relieving symptoms associated with ASD, their preliminary nature does not allow any definitive conclusions to be drawn concerning potential therapeutic exploitation.”
Doenni VM, Gray JM, Song CM, Patel S, Hill MN, Pittman QJ. Deficient adolescent social behavior following early-life inflammation is ameliorated by augmentation of anandamide signaling. Brain Behav Immun 2016;58:237-247.
Inflammation was induced in 14-day old rats with administration of a lipopolysaccharide. Control rats received a saline injection. Subsequent differences in social behavior tests and in endocannabinoid system were studied. LPS-injected rats exhibited a lower level of social behavior. Oral administration of an inhibitor of the enzyme that degrades the endocannabinoid AEA resulted in none of the social behavior impairment expected in LPS-injected rats. Control rats were unaffected.
Servadio M, Melancia F, Manduca A, di Masi A, Schlavi S, et al. Targeting anandamide metabolism rescues core and associated autistic-like symptoms in rats prenatally exposed to valproic acid. Transl Psychiatry 2016;6 e902 doi:10.1038/tp.20616.182.
The following is from the article’s abstract. Anandamide is one of the primary endocannabinoids. “VPA-exposed rats showed early deficits in social communication and discrimination, compromised sociability and social play behavior, stereotypies and increased anxiety, thus providing preclinical proof of the long-lasting deleterious effects induced by prenatal VPA exposure. At the neurochemical level, VPA-exposed rats displayed altered phosphorylation of CB1 cannabinoid receptors in different brain areas, associated with changes in anandamide metabolism from infancy to adulthood. Interestingly, enhancing anandamide signaling through inhibition of it degradation rescued the behavioral deficits displayed by VPA- exposed rats at infancy, adolescence and adulthood. This study therefore shows that abnormalities in anandamide activity may underlie the deleterious impact of environmental risk factors on ASD-relevant behaviors and that the endocannabinoid system may represent a therapeutic target for the core and associated symptoms displayed by autistic patients.”
Wei D, Dinh D, Lee D, Anguren A, Moreno-Sanz G, et al. Enhancement of anandamide- mediated endocannabinoid signaling corrects autism-related social impairment. Cannabis and Cannabinoid Research 2016;1:1, 81-89, DOI:10.1089/can.2015.0008.
Effect of administering an inhibitor of the enzyme that degrades the endocannabinoid AEA was tested on two distinct mouse models of ASD. The two models were a strain with a mutation that models human Fragile-X Syndrome and the BTRT mouse strain – an inbred strain with behaviors similar to ASD not known to be caused by a mutation. Social impairment was tested with a previously established method: the three-chambered social approach task. First the mice were habituated to the center chamber for ten minutes with the doors to the other two chambers closed. Then the mice were tested in a ten-minute session. Subjects were offered a choice between a novel object and a novel mouse in opposing side chambers. The novel object was a clear, empty inverted pencil cup and the novel social stimulus mouse was a sex, age, and weight-matched mouse constrained by a clear, empty inverted pencil cup. Chamber time scoring was automated using image analysis. Sniffing time was scored by trained assistants who were unaware of treatment conditions. Administration of a drug that inhibits FAAH, an enzyme that degrades AEA, completely reversed the social impairment found in both strains.
Clinical Trials
No randomized, controlled clinical trials have been completed for cannabis or cannabinoids as therapy for ASD. However, two have been registered on www.clinicaltrials.gov. and are now under way (see descriptions below). Though internet blogs and discussion forums have numerous accounts of use of cannabis and cannabinoids in persons with autism, the following case history was the only publication found for therapeutic use of a cannabinoid or cannabis product for autism.
Kurz R, Blaas. Use of dronabinol (delta-9-THC) in autism: a prospective single- case-study with an early infantile autistic child. Cannabinoids 2010;5:4-6.
In this study, synthetic delta-9-THC (dronabinol) was studied as a supplemental therapy in an autistic Austrian child. The child at the center of this study was diagnosed with early infantile autism at the age of three. He was six years old when the study was conducted. The study lasted six months. During the study period, the child initially received dronabinol drops at a dosage of one drop every morning (0.62 mg THC). On a day-to-day basis, the dosage was gradually increased, reaching a maximum tolerated dose of 3.62 mg THC per day (two drops in the morning, one drop at midday, and three evening drops).
At the end of the six months, the boy’s symptom severity significantly decreased in five different categories: hyperactivity, lethargy, irritability, stereotypic behavior, and inappropriate speech. Based on these findings, the authors argue that dronabinol may be a therapeutic for treating early infantile autism. Dronabinol may not replace other therapies, but it is a potential, additional therapy. Larger, controlled studies on cannabinoids and autism are needed to further understand their findings, say the authors.
Cannabinoids for Behavioral Problems in Children with ASD (CBA): NCT02956226 (registered on www.clinicaltrials.gov)
This is a double blind randomized placebo-controlled clinical trial of two cannabis formulations to treat disruptive behaviors in children and young adults (age 5-21) with ASD. It is being carried out in Israel. Estimated enrollment is 120 patients, who will be assigned to one of three olive oil-based solutions for a three-month treatment period: 1) 99% CBD and 99% THC in a ratio of 20:1 CBD:THC; 2) whole plant extract with a CBD:THC ratio of 20:1; or, 3) placebo. Primary outcome is change from baseline Home Situations Questionnaire-Autism Spectrum Disorder score, at 3 months (it is a 24-item parent-rated measure of noncompliant behavior in children with ASD). There are several other outcome measures. Recruitment began January, 2017. Estimated study completion date is July, 2019.
Cannabidivarin (CBDV) vs. Placebo in Children with Autism Spectrum Disorder (ASD): NCT03202303 (registered on www.clinicaltrials.gov)
This double blind placebo-controlled clinical trial of CBDV to treat children (age 5-18 years) will be carried out in New York City. Estimated enrollment is 100 patients, who will be assigned to either 800 mg/day (400 mg twice/day) CBDV or placebo capsule for a 12-week treatment period. Primary outcome is change from baseline Aberrant Behavior Checklist-Irritability Subscale, at 12 weeks. There are several other outcome measures. Recruitment will begin October, 2017. Estimated study completion date is September, 2021.
Observational Studies
De Alwis D, Agrawal A, Reiersen AM, Constantino JN, Henders A, Martin NG, & Lynskey MT. ADHD symptoms, autistic traits, and substance use and misuse in adult Australian twins. J Stud Alcohol Drugs 2014;75:211-221.
Substance use among people with autism spectrum disorders (ASD) is hypothesized to be rare, since those with ASD lack the social skills that would bring them into contact with others who use drugs and since people with ASD have less novelty-seeking behaviors than average. However, there are few studies to test this hypothesis. This study uses a cross- sectional interview and self-reported questionnaire to elucidate the relationship between people with autism traits, substance use, and substance abuse. The interview and questionnaire study sample size was 3,028 white, Australian twins born between 1972 and 1979. The study participants’ drug use, abuse, and misuse were assessed through the interview. The self- reported questionnaire collected data on the participants’ autistic traits.
Surprisingly, the results of the analysis indicate that cannabis use is associated with having autistic traits in a statistically significant manner. Cannabis abuse/dependence were also significantly associated with high levels of autistic traits.
Several factors limit interpretation of this finding, however. From a demographic perspective, the study sample is racially homogenous, and its findings may not be replicated in more diverse study samples. Causal relationships cannot be determined because of the study’s cross-sectional design. Last, formal diagnostic criteria were not used to determine an autism spectrum disorder diagnosis: only autistic traits were studied.
National Medical Organization Recommendations
No guidance documents or recommendations from national medical organizations for the therapeutic use of cannabis or cannabinoids in the management of autism spectrum disorder were found.
References
American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing, 2013.
Buescher AV, Cidav Z, Knapp M, Mandell DS. Costs of autism spectrum disorders in the United Kingdom and the United States. JAMA Pediatr 2014;168:721-728.
Christensen DL, Baio J, Van Naarden BK, Bilder D, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2012. MMWR Surveill Summ 2016;65:1-23.
De Alwis D, Agrawal A, Reiersen AM, Constantino JN, Henders A, Martin NG, Lynskey MT. ADHD symptoms, autistic traits, and substance use and misuse in adult Australian twins. J Stud Alcohol Drugs 2014;75:211-221.
Doenni VM, Gray JM, Song CM, Patel S, Hill MN, Pittman QJ. Deficient adolescent social behavior following early-life inflammation is ameliorated by augmentation of anandamide signaling. Brain Behav Immun 2016;58:237-247.
Dove D, Warren Z, McPheeters ML, Taylor JL, Sathe NA, Veenstra-VanderVeele J. Medications for adolescents and young adults with autism spectrum disorders: A systematic review. Pediatrics 2012;130:717-726.
Hanley GP, Iwata BA, Thompson RH. Reinforcement schedule thinning following treatment with functional communication training. J Applied Behav Anal 2001;34:17-38.
Harrington JW, Allen K. The clinician's guide to autism. Pediatr Rev 2014;35:62-78.
Kurz R, Blaas K. Use of dronabinol (delta-9-THC) in autism: a prospective single-case-study with an early infantile autistic child. Cannabinoids 2010;5:4-6.
Lovaas, O. I. Behavioral treatment and normal educational and intellectual functioning in young autistic children. J Consult Clin Psychol 1987;55:3-9.
McPheeters ML, Warren Z, Sathe N, Bruzek JL, Krishnaswami S, Jerome RN, Veenstra- VanderWeele J. A systematic review of medical treatments for children with autism spectrum disorders. Pediatrics 2011;127:e1312-e1321.
Ospina MB, Seida JK, Clark B, Karkhaneh M, Hartling L, Tjosvold L, et al. Behavioural and developmental interventions for autism spectrum disorder: a clinical systematic review. PloS One 2008;3(11), e3755.
Servadio M, Melancia F, Manduca A, di Masi A, Schlavi S, et al. Targeting anandamide metabolism rescues core and associated autistic-like symptoms in rats prenatally exposed to valproic acid. Transl Psychiatry 2016;6 e902 doi:10.1038/tp.20616.182.
Taylor JL, Dove D, Veenstra-VanderWeele J, Sathe NA, McPheeters ML, Jerome RN, Warren Z. Interventions for adolescents and young adults with autism spectrum disorders. Comparative Effectiveness Review, Agency for Healthcare Research and Quality (US) 2012;65.
Warren Z, McPheeters ML, Sathe N, Foss-Feig JH, Glasser A, Veenstra-VanderWeele J. A systematic review of early intensive intervention for autism spectrum disorders. Pediatrics 2011;127:e1303-1311.
Wei D, Dinh D, Lee D, Anguren A, Moreno-Sanz G, et al. Enhancement of anandamide-mediated endocannabinoid signaling corrects autism-related social impairment. Cannabis and Cannabinoid Research 2016;1:1, 81-89, DOI:10.1089/can.2015.0008.
White SW, Keonig K, Scahill L. Social skills development in children with autism spectrum disorders: A review of the intervention research. J Autism Dev Disord 2007;37:1858-1868. Zamberletti E, Gabaglio M, Parolaro D. The endocannabinoid system and autism spectrum disorders: Insights from animals. Int J Mol Sci 2017;18(9). pii: E1916. doi: 10.3390/ijms1809191
PDF Link: http://www.health.state.mn.us/topics/cannabis/rulemaking/autismbrief2.pdf
Source: Minnesota Department of Health
PO Box 64882
St. Paul, MN 55164-0882
651-201-5598
health.cannabis@state.mn.us | http://www.health.state.mn.us/topics/cannabis
09/2017 | To obtain this information in a different format, call: 651-201-5598.
Dr. Dustin Sulak is respected as a top cannabis educator for good reason – he’s been on the frontlines for several years, working with medical cannabis patients in Maine.
Interview with Dr. Dustin Sulak (DS) on Medical Cannabis and Autism
Green Flower Media(GF) : What are your thoughts on treating autism with cannabis?
Dustin Sulak: The underlying pathology in autism is complex and poorly understood, but we do know that it includes inappropriate inflammation and dysfunction in the central nervous system and gut.
We currently don’t have many treatments that are effective. The best-case scenario would be to find a treatment that is safe, decreases inflammation, protects and promotes healing in the nervous system and gut, and helps manage the most severe symptoms of autism.
Cannabis seems to fit that description.
GF: Any case studies you like to share from your own clinical experience?
DS: How about the case I presented at the 2016 Cannabis Health Summit of the 12-year-old boy, who was in the ER for a week with severe self-injurious behavior before getting 5mg THC and walking out giggling a few hours later.
His symptoms were so severe he had to be restrained much of the time, and no hospital in New England could place him.
I finally convinced the ER doc to give him 5 mg dronabinol [an FDA-approved synthetic version of isolated THC) since he had previously responded well to an equivalent dose of cannabis brownies.
The latest batch of brownies must have been weaker than the previous – that’s our best guess for why he stopped responding and had to go to the ER.
He had severe self-injurious behavior (putting his head through walls) and has been stable on a low dose THC for three years.
Now he’s employed in a salsa company, grilling veggies, and lives a productive and self-injury-free life.
I had another interesting case of a 22-year-old with autism and aggression episodes who was minimally verbal – one word responses only. When he first tried cannabis he had a remarkable two-week period when he was speaking complete sentences.
This improvement gradually regressed and he is now back to his baseline speech, but cannabis still helps him with behavioral issues.
I’m not sure if there was something special about his initial dose (unlabeled and untested oil), but we have been unable to reproduce the benefit thus far.
I have another case of a 12-year-old boy who does well with cannabis but he requires an incredibly high dose: 50-200mg THC required to help him settle down to sleep or to stimulate appetite and focus on meals.
My sensitization protocol does not change these high-dose requirements. He shows no signs of impairment or intoxication at these doses. CBD doesn’t have much of an effect on him.
GF: Do you think treating autism with cannabis is more of a behavioral therapy or are we looking at targeting the endocannabinoid system and cannabinoid signaling?
DS: I think we have both, which is so often the case with cannabis. It helps ameliorate symptoms, especially the most severe symptoms like self-injury or aggressive behavior and low appetite/weight loss.
It can also help improve communication and cooperation – it appears to me that my autistic patients feel more comfortable in their bodies with the help of cannabis, and are more likely to make eye contact, initiate interaction, and even give hugs.
At the same time, it’s likely (but unproven) that long-term treatment could address the underlying pathology to some extent by protecting the nervous system, promoting neuroplasticity, and reducing inflammation.
GF: What would you say to parents or patients struggling with autism?
DS: For severe behavioral symptoms, and even mild ones, don’t be afraid to try THC. While I’m excited to see what we can learn about CBD in autism, I want to clearly dispel the myth that CBD is the medical part and THC is the recreational part of the plant.
Based on my clinical experience, THC is well tolerated and very effective in autism. Like most other conditions, it’s likely that some combination of THC and CBD will be best for most patients.
I encourage parents to set concrete goals of treatment. Some of the parents I work with will stop at nothing to help their child become neurotypical.
While that may be possible, I like to identify high impact goals that can improve quality of life and work towards those. It’s very hard on a parent-child relationship for the child to always be perceived as broken and needing fixing.
I tell my parents to look right past the dysfunctions and problems when they can, and see the health and beauty in their children.
When they do that, every interaction becomes a healing event for both parent and child.
While cannabis is an incredible medicine, love may be even be even stronger.
Interview Source: Green Flower Media 9/2017
Source:
[https://www.learngreenflower.com/articles/508/interview-cannabis-doctor-speaks-out-on-autism]
Autism is a neurodevelopmental disorder that develops in infancy or childhood. The disorder is characterized by social interaction and communications impairments, as well as restricted and repetitive behaviors. Studies have shown cannabis is effective at improving behavior and communication abilities by repairing the brain’s ability to send clear signals.
Symptoms must be present in the early developmental period. Though, symptoms may not become fully apparent until social demands exceed limited capacities. Symptoms may also be masked by learned strategies in later life.
Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and autism spectrum disorder frequently co-occur. Social communication should be below what is expected for general developmental level, in order to make comorbid diagnoses of autism spectrum disorder and intellectual disability
Prevalence
The Centers for Disease Control and Prevention estimates that 1 out of every 68 children in the United States has autism spectrum disorder. ASD is roughly 4.5 times more common among boys than girls (Christensen 2016). Since 2006, the prevalence of childhood ASD has increased by 23%, becoming a major public-health concern. This increase in prevalence can be attributed to better screening and the DSM-5’s broader definition of ASD, among other issues (Harrington and Allen 2014).
Among both children and adults, roughly 3.5 million Americans live with autism spectrum disorder. Annually, costs associated with children who have ASD are $61 billion in the United States. Adults living with ASD cost the U.S. $196 billion per year (Buescher 2014).
Current Therapies
Several behavioral, educational, and pharmaceutical treatments are used to manage ASD. Pharmaceutical treatments mostly target comorbid health problems, which are common in children living with ASD (McPheeters 2011).
Behavioral and developmental interventions are the primary treatments for ASD (Ospina 2008). There is a great variety in the kinds of behavioral and developmental interventions, which are organized into smaller subcategories (Ospina 2008). For example, within the continuum of behavioral and developmental interventions, applied behavioral analysis (ABA) is designed to teach socially appropriate behaviors and to decrease challenging behaviors (Harrington 2014, Ospina 2008). Another kind of behavior and developmental intervention is social skills training (SST), which targets social deficits (White 2007).
ABA-based therapies have demonstrated positive effects on language, adaptive, cognitive, and educational outcomes (Hanley 2001, Lovaas 1987, Warren 2011). However, there is a lack of high-quality randomized controlled trials (Warren 2011). The studies that do evaluate behavioral and developmental interventions are methodologically weak, include few participants, and do not evaluate long-term effects of interventions (Ospina 2008). Therefore, the evidence to determine which behavioral interventions are most effective in children with ASD is inadequate (Warren et al., 2011). Studies on SST interventions are similarly low-quality, though evidence from several small, initial studies indicate that SST is potentially beneficial to children with ASD (White 2007).
Common comorbidities in children with ASD include intellectual disability, constipation, sleep disorders, anxiety, ADHD, and seizure disorders (Harrington and Allen, 2014; McPheeters 2011). Treating comorbid mental-health issues in children with ASD is more challenging than treating common medical problems, such as constipation and sleep problems (Harrington 2014). Antipsychotic medications, serotonin-reuptake inhibitors, and stimulants are among the pharmaceuticals used to treat mental-health comorbidities (McPheeters 2011). However, despite the fact that medications are used to treat many children with ASD, there is little evidence to indicate that these pharmaceuticals are effective (McPheeters 2011). Drugs that do demonstrate benefits for challenging or repetitive behaviors, are unfortunately associated with adverse effects, limiting their use to patients with severe impairments or risk of injury (McPheeters 2011).
Turning to adolescents and young adults with ASD, studies examining the effectiveness of behavioral, pharmaceutical, and other therapies in this population are poor-quality (Taylor 2012). There is a dramatic lack of evidence on the best way to treat adolescents and young adults who have ASD (Dove 2012, Taylor 2012).
Pre-Clinical Research
A September, 2017 review by Zamberletti et al (Zamberletti 2017) provides a good overview of the lines of evidence from animal studies suggesting the endocannabinoid system (ECS) plays a role in autism. Recently, at least three articles (Doenni 206, Servadio 2016, and Wei 2016) have reported on studies that manipulated the ECS in mouse models of autism.
Zamberletti E, Gabaglio M, Parolaro D. The endocannabinoid system and autism spectrum disorders: Insights from animals. Int J Mol Sci 2017;18(9). pii: E1916. doi: 10.3390/ijms18091916
This review provides evidence of involvement of the ECS in autism through modulation of autism-like behaviors and research suggesting possible mechanisms of action.
Genetic-based models:
Fragile X syndrome (FXS) is the most common known genetic cause of ASD. A mouse model of FXS has been developed: the Fmr1 knockout mouse. Fmr1 mice have been shown to have dysregulated endocannabinoid signaling. And studies that inhibited different enzymes that degrade endocannabinoids showed improvement in autism- consistent behaviors.
Inbreeding has produced a group of mouse strains used as a model for idiopathic (cause unknown) autism because the mice exhibit behaviors consistent with those seen in humans with ASD, but with no known gene mutation causing the behaviors. Prominent among these strains is the BTBR mouse model. Treatment to increase the level of one endocannabinoid (AEA) resulted in reduced ASD-like behavior.
Environmental-based models – environmental manipulations in rodents conducted using the same agents that have been correlated with human autism:
The valproic acid (VPA) rat model has been used extensively to evaluate the possible involvement of the endocannabinoid system in ASD. VPA is an anti-epileptic drug. Several studies have shown use of VPA during pregnancy may cause neural tube defects and cognitive impairment in children. In animal studies, offspring of rats administered VPA during pregnancy show lower social interaction, increased repetitive/sterotyped behaviors, early signs of neurodevelopment impairment, and abnormal responses to painful and non-painful stimuli. Studies have been done administering to rats exposed to VPA in utero substances that inhibit the breakdown of an endocannabinoid (AEA). Results showed decrease in the autism-model behaviors, with greater decrease seen in males.
Both viral and bacterial infections during pregnancy have been linked to an increased risk to develop ASD in the offspring. Injection of pregnant rodents with the substance, polyinosine:cytosine (LPS), which mimics the immune activation seen with the influenza virus, produces ASD-like behaviors in the offspring. These include impairments in social interaction and communication, stereotyped patterns of behavior, anxiety, and impaired learning and memory. These behaviors in the offspring were accompanied by distinctive changes in brain neuron structure and function. The tie to the endocannabinoid system comes with studies that administered LPS to rodents soon after birth. This resulted in decreased social play, reduced CB1 (cannabinoid receptor 1) binding, and increased levels of the endocannabinoid, AEA.
Possible mechanisms of action:
Studies have shown elements of the ECS interact with oxytocin, a neuropeptide that promotes parental and social bonding. Oxytocin stimulates endocannabinoid release in a relevant part of the brain (nucleus accumbens) and there is evidence endocannabinoid signaling is required for the prosocial effects of oxytocin.
mTOR signaling is involved in memory consolidation and normalization of mTOR signaling in the hippocampus reduces the cognitive deficits caused by cannabinoid receptor 1 blockade of Fmr1 (fragile X Syndrome model) mice. Dysregulation of mTOR signaling appears to be a feature common to a subset of ASD. (mTOR is an enzyme that controls cell growth and metabolism).
There is evidence that endocannabinoids might modulate ASD symptoms via interaction with immune system cells. Changes in endocannabinoid metabolism and in expression cannabinoid receptors (CB2) on certain white blood cells have been seen in ASD patients.
The authors conclude, “Although preclinical findings seem to suggest that pharmacological interventions aimed at modulating the EC system could be beneficial for relieving symptoms associated with ASD, their preliminary nature does not allow any definitive conclusions to be drawn concerning potential therapeutic exploitation.”
Doenni VM, Gray JM, Song CM, Patel S, Hill MN, Pittman QJ. Deficient adolescent social behavior following early-life inflammation is ameliorated by augmentation of anandamide signaling. Brain Behav Immun 2016;58:237-247.
Inflammation was induced in 14-day old rats with administration of a lipopolysaccharide. Control rats received a saline injection. Subsequent differences in social behavior tests and in endocannabinoid system were studied. LPS-injected rats exhibited a lower level of social behavior. Oral administration of an inhibitor of the enzyme that degrades the endocannabinoid AEA resulted in none of the social behavior impairment expected in LPS-injected rats. Control rats were unaffected.
Servadio M, Melancia F, Manduca A, di Masi A, Schlavi S, et al. Targeting anandamide metabolism rescues core and associated autistic-like symptoms in rats prenatally exposed to valproic acid. Transl Psychiatry 2016;6 e902 doi:10.1038/tp.20616.182.
The following is from the article’s abstract. Anandamide is one of the primary endocannabinoids. “VPA-exposed rats showed early deficits in social communication and discrimination, compromised sociability and social play behavior, stereotypies and increased anxiety, thus providing preclinical proof of the long-lasting deleterious effects induced by prenatal VPA exposure. At the neurochemical level, VPA-exposed rats displayed altered phosphorylation of CB1 cannabinoid receptors in different brain areas, associated with changes in anandamide metabolism from infancy to adulthood. Interestingly, enhancing anandamide signaling through inhibition of it degradation rescued the behavioral deficits displayed by VPA- exposed rats at infancy, adolescence and adulthood. This study therefore shows that abnormalities in anandamide activity may underlie the deleterious impact of environmental risk factors on ASD-relevant behaviors and that the endocannabinoid system may represent a therapeutic target for the core and associated symptoms displayed by autistic patients.”
Wei D, Dinh D, Lee D, Anguren A, Moreno-Sanz G, et al. Enhancement of anandamide- mediated endocannabinoid signaling corrects autism-related social impairment. Cannabis and Cannabinoid Research 2016;1:1, 81-89, DOI:10.1089/can.2015.0008.
Effect of administering an inhibitor of the enzyme that degrades the endocannabinoid AEA was tested on two distinct mouse models of ASD. The two models were a strain with a mutation that models human Fragile-X Syndrome and the BTRT mouse strain – an inbred strain with behaviors similar to ASD not known to be caused by a mutation. Social impairment was tested with a previously established method: the three-chambered social approach task. First the mice were habituated to the center chamber for ten minutes with the doors to the other two chambers closed. Then the mice were tested in a ten-minute session. Subjects were offered a choice between a novel object and a novel mouse in opposing side chambers. The novel object was a clear, empty inverted pencil cup and the novel social stimulus mouse was a sex, age, and weight-matched mouse constrained by a clear, empty inverted pencil cup. Chamber time scoring was automated using image analysis. Sniffing time was scored by trained assistants who were unaware of treatment conditions. Administration of a drug that inhibits FAAH, an enzyme that degrades AEA, completely reversed the social impairment found in both strains.
Clinical Trials
No randomized, controlled clinical trials have been completed for cannabis or cannabinoids as therapy for ASD. However, two have been registered on www.clinicaltrials.gov. and are now under way (see descriptions below). Though internet blogs and discussion forums have numerous accounts of use of cannabis and cannabinoids in persons with autism, the following case history was the only publication found for therapeutic use of a cannabinoid or cannabis product for autism.
Kurz R, Blaas. Use of dronabinol (delta-9-THC) in autism: a prospective single- case-study with an early infantile autistic child. Cannabinoids 2010;5:4-6.
In this study, synthetic delta-9-THC (dronabinol) was studied as a supplemental therapy in an autistic Austrian child. The child at the center of this study was diagnosed with early infantile autism at the age of three. He was six years old when the study was conducted. The study lasted six months. During the study period, the child initially received dronabinol drops at a dosage of one drop every morning (0.62 mg THC). On a day-to-day basis, the dosage was gradually increased, reaching a maximum tolerated dose of 3.62 mg THC per day (two drops in the morning, one drop at midday, and three evening drops).
At the end of the six months, the boy’s symptom severity significantly decreased in five different categories: hyperactivity, lethargy, irritability, stereotypic behavior, and inappropriate speech. Based on these findings, the authors argue that dronabinol may be a therapeutic for treating early infantile autism. Dronabinol may not replace other therapies, but it is a potential, additional therapy. Larger, controlled studies on cannabinoids and autism are needed to further understand their findings, say the authors.
Cannabinoids for Behavioral Problems in Children with ASD (CBA): NCT02956226 (registered on www.clinicaltrials.gov)
This is a double blind randomized placebo-controlled clinical trial of two cannabis formulations to treat disruptive behaviors in children and young adults (age 5-21) with ASD. It is being carried out in Israel. Estimated enrollment is 120 patients, who will be assigned to one of three olive oil-based solutions for a three-month treatment period: 1) 99% CBD and 99% THC in a ratio of 20:1 CBD:THC; 2) whole plant extract with a CBD:THC ratio of 20:1; or, 3) placebo. Primary outcome is change from baseline Home Situations Questionnaire-Autism Spectrum Disorder score, at 3 months (it is a 24-item parent-rated measure of noncompliant behavior in children with ASD). There are several other outcome measures. Recruitment began January, 2017. Estimated study completion date is July, 2019.
Cannabidivarin (CBDV) vs. Placebo in Children with Autism Spectrum Disorder (ASD): NCT03202303 (registered on www.clinicaltrials.gov)
This double blind placebo-controlled clinical trial of CBDV to treat children (age 5-18 years) will be carried out in New York City. Estimated enrollment is 100 patients, who will be assigned to either 800 mg/day (400 mg twice/day) CBDV or placebo capsule for a 12-week treatment period. Primary outcome is change from baseline Aberrant Behavior Checklist-Irritability Subscale, at 12 weeks. There are several other outcome measures. Recruitment will begin October, 2017. Estimated study completion date is September, 2021.
Observational Studies
De Alwis D, Agrawal A, Reiersen AM, Constantino JN, Henders A, Martin NG, & Lynskey MT. ADHD symptoms, autistic traits, and substance use and misuse in adult Australian twins. J Stud Alcohol Drugs 2014;75:211-221.
Substance use among people with autism spectrum disorders (ASD) is hypothesized to be rare, since those with ASD lack the social skills that would bring them into contact with others who use drugs and since people with ASD have less novelty-seeking behaviors than average. However, there are few studies to test this hypothesis. This study uses a cross- sectional interview and self-reported questionnaire to elucidate the relationship between people with autism traits, substance use, and substance abuse. The interview and questionnaire study sample size was 3,028 white, Australian twins born between 1972 and 1979. The study participants’ drug use, abuse, and misuse were assessed through the interview. The self- reported questionnaire collected data on the participants’ autistic traits.
Surprisingly, the results of the analysis indicate that cannabis use is associated with having autistic traits in a statistically significant manner. Cannabis abuse/dependence were also significantly associated with high levels of autistic traits.
Several factors limit interpretation of this finding, however. From a demographic perspective, the study sample is racially homogenous, and its findings may not be replicated in more diverse study samples. Causal relationships cannot be determined because of the study’s cross-sectional design. Last, formal diagnostic criteria were not used to determine an autism spectrum disorder diagnosis: only autistic traits were studied.
National Medical Organization Recommendations
No guidance documents or recommendations from national medical organizations for the therapeutic use of cannabis or cannabinoids in the management of autism spectrum disorder were found.
References
American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing, 2013.
Buescher AV, Cidav Z, Knapp M, Mandell DS. Costs of autism spectrum disorders in the United Kingdom and the United States. JAMA Pediatr 2014;168:721-728.
Christensen DL, Baio J, Van Naarden BK, Bilder D, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2012. MMWR Surveill Summ 2016;65:1-23.
De Alwis D, Agrawal A, Reiersen AM, Constantino JN, Henders A, Martin NG, Lynskey MT. ADHD symptoms, autistic traits, and substance use and misuse in adult Australian twins. J Stud Alcohol Drugs 2014;75:211-221.
Doenni VM, Gray JM, Song CM, Patel S, Hill MN, Pittman QJ. Deficient adolescent social behavior following early-life inflammation is ameliorated by augmentation of anandamide signaling. Brain Behav Immun 2016;58:237-247.
Dove D, Warren Z, McPheeters ML, Taylor JL, Sathe NA, Veenstra-VanderVeele J. Medications for adolescents and young adults with autism spectrum disorders: A systematic review. Pediatrics 2012;130:717-726.
Hanley GP, Iwata BA, Thompson RH. Reinforcement schedule thinning following treatment with functional communication training. J Applied Behav Anal 2001;34:17-38.
Harrington JW, Allen K. The clinician's guide to autism. Pediatr Rev 2014;35:62-78.
Kurz R, Blaas K. Use of dronabinol (delta-9-THC) in autism: a prospective single-case-study with an early infantile autistic child. Cannabinoids 2010;5:4-6.
Lovaas, O. I. Behavioral treatment and normal educational and intellectual functioning in young autistic children. J Consult Clin Psychol 1987;55:3-9.
McPheeters ML, Warren Z, Sathe N, Bruzek JL, Krishnaswami S, Jerome RN, Veenstra- VanderWeele J. A systematic review of medical treatments for children with autism spectrum disorders. Pediatrics 2011;127:e1312-e1321.
Ospina MB, Seida JK, Clark B, Karkhaneh M, Hartling L, Tjosvold L, et al. Behavioural and developmental interventions for autism spectrum disorder: a clinical systematic review. PloS One 2008;3(11), e3755.
Servadio M, Melancia F, Manduca A, di Masi A, Schlavi S, et al. Targeting anandamide metabolism rescues core and associated autistic-like symptoms in rats prenatally exposed to valproic acid. Transl Psychiatry 2016;6 e902 doi:10.1038/tp.20616.182.
Taylor JL, Dove D, Veenstra-VanderWeele J, Sathe NA, McPheeters ML, Jerome RN, Warren Z. Interventions for adolescents and young adults with autism spectrum disorders. Comparative Effectiveness Review, Agency for Healthcare Research and Quality (US) 2012;65.
Warren Z, McPheeters ML, Sathe N, Foss-Feig JH, Glasser A, Veenstra-VanderWeele J. A systematic review of early intensive intervention for autism spectrum disorders. Pediatrics 2011;127:e1303-1311.
Wei D, Dinh D, Lee D, Anguren A, Moreno-Sanz G, et al. Enhancement of anandamide-mediated endocannabinoid signaling corrects autism-related social impairment. Cannabis and Cannabinoid Research 2016;1:1, 81-89, DOI:10.1089/can.2015.0008.
White SW, Keonig K, Scahill L. Social skills development in children with autism spectrum disorders: A review of the intervention research. J Autism Dev Disord 2007;37:1858-1868. Zamberletti E, Gabaglio M, Parolaro D. The endocannabinoid system and autism spectrum disorders: Insights from animals. Int J Mol Sci 2017;18(9). pii: E1916. doi: 10.3390/ijms1809191
PDF Link: http://www.health.state.mn.us/topics/cannabis/rulemaking/autismbrief2.pdf
Source: Minnesota Department of Health
PO Box 64882
St. Paul, MN 55164-0882
651-201-5598
health.cannabis@state.mn.us | http://www.health.state.mn.us/topics/cannabis
09/2017 | To obtain this information in a different format, call: 651-201-5598.
Interview: Medical Cannabis Doctor Speaks Out on Autism
Dr. Dustin Sulak is respected as a top cannabis educator for good reason – he’s been on the frontlines for several years, working with medical cannabis patients in Maine.
Interview with Dr. Dustin Sulak (DS) on Medical Cannabis and Autism
Green Flower Media(GF) : What are your thoughts on treating autism with cannabis?
Dustin Sulak: The underlying pathology in autism is complex and poorly understood, but we do know that it includes inappropriate inflammation and dysfunction in the central nervous system and gut.
We currently don’t have many treatments that are effective. The best-case scenario would be to find a treatment that is safe, decreases inflammation, protects and promotes healing in the nervous system and gut, and helps manage the most severe symptoms of autism.
Cannabis seems to fit that description.
GF: Any case studies you like to share from your own clinical experience?
DS: How about the case I presented at the 2016 Cannabis Health Summit of the 12-year-old boy, who was in the ER for a week with severe self-injurious behavior before getting 5mg THC and walking out giggling a few hours later.
His symptoms were so severe he had to be restrained much of the time, and no hospital in New England could place him.
I finally convinced the ER doc to give him 5 mg dronabinol [an FDA-approved synthetic version of isolated THC) since he had previously responded well to an equivalent dose of cannabis brownies.
The latest batch of brownies must have been weaker than the previous – that’s our best guess for why he stopped responding and had to go to the ER.
He had severe self-injurious behavior (putting his head through walls) and has been stable on a low dose THC for three years.
Now he’s employed in a salsa company, grilling veggies, and lives a productive and self-injury-free life.
I had another interesting case of a 22-year-old with autism and aggression episodes who was minimally verbal – one word responses only. When he first tried cannabis he had a remarkable two-week period when he was speaking complete sentences.
This improvement gradually regressed and he is now back to his baseline speech, but cannabis still helps him with behavioral issues.
I’m not sure if there was something special about his initial dose (unlabeled and untested oil), but we have been unable to reproduce the benefit thus far.
I have another case of a 12-year-old boy who does well with cannabis but he requires an incredibly high dose: 50-200mg THC required to help him settle down to sleep or to stimulate appetite and focus on meals.
My sensitization protocol does not change these high-dose requirements. He shows no signs of impairment or intoxication at these doses. CBD doesn’t have much of an effect on him.
GF: Do you think treating autism with cannabis is more of a behavioral therapy or are we looking at targeting the endocannabinoid system and cannabinoid signaling?
DS: I think we have both, which is so often the case with cannabis. It helps ameliorate symptoms, especially the most severe symptoms like self-injury or aggressive behavior and low appetite/weight loss.
It can also help improve communication and cooperation – it appears to me that my autistic patients feel more comfortable in their bodies with the help of cannabis, and are more likely to make eye contact, initiate interaction, and even give hugs.
At the same time, it’s likely (but unproven) that long-term treatment could address the underlying pathology to some extent by protecting the nervous system, promoting neuroplasticity, and reducing inflammation.
GF: What would you say to parents or patients struggling with autism?
DS: For severe behavioral symptoms, and even mild ones, don’t be afraid to try THC. While I’m excited to see what we can learn about CBD in autism, I want to clearly dispel the myth that CBD is the medical part and THC is the recreational part of the plant.
Based on my clinical experience, THC is well tolerated and very effective in autism. Like most other conditions, it’s likely that some combination of THC and CBD will be best for most patients.
I encourage parents to set concrete goals of treatment. Some of the parents I work with will stop at nothing to help their child become neurotypical.
While that may be possible, I like to identify high impact goals that can improve quality of life and work towards those. It’s very hard on a parent-child relationship for the child to always be perceived as broken and needing fixing.
I tell my parents to look right past the dysfunctions and problems when they can, and see the health and beauty in their children.
When they do that, every interaction becomes a healing event for both parent and child.
While cannabis is an incredible medicine, love may be even be even stronger.
Interview Source: Green Flower Media 9/2017
Source:
[https://www.learngreenflower.com/articles/508/interview-cannabis-doctor-speaks-out-on-autism]
Petition Research About Medical Cannabis and Autism Spectrum Disorders
OVERVIEW OF AUTISM
Autism spectrum disorder (ASD) is a term used to classify a range of complex neurodevelopment disorders that are characterized, in varying degrees, by social interaction difficulties, verbal and physical communication problems, and restricted and repetitive patterns of behavior. Of the numerous types of ASD’s is autism, also referred to as “classical ASD.” Autism is the most severe form of ASD. Other types of ASD’s include Asperger syndrome, childhood disintegrative disorder, and pervasive developmental disorder-not otherwise specified. According to the National Institute of Neurological Disorders and Stroke, 1 out of 88 children age 8 will have an ASD and males are four times more likely to have one of the disorders than females.
Impaired social interaction is the main sign of ASD and it can become visible as early as infancy. Babies and children with ASD can be unresponsive to people, avoid eye contact or fail to respond to their names. They may focus on one item for a long period of time without noticing any outside stimulation. They struggle at interpreting the thoughts and feelings of others and therefore have problems understanding and responding to social cues like facial expressions and tone of voice. It’s not uncommon for them to lack empathy. Repetitive motions like rocking or twirling, or self-abusive behaviors, like biting or head banging, are common in children with autism.
Very early indicators of an ASD include not responding to one’s name, poor eye contact, no babbling or pointing by age 1, no single words by 16 months, excessive lining up of toys or other objects and no smiling or social responsiveness. Later indicators include an impaired ability to make friends, difficulty initiating or sustaining a conversation, impaired imaginative play, repetitive or unusual language, restricted patterns of focus and the inflexible need to stick with routines.
The causes of ASD are unknown, but according to the National Institute of Neurological Disorders and Stroke, both genetics and environment likely play a role. Brain irregularities and abnormal neurotransmitter levels are commonly found in ASD infants and children, which suggest that the disease is caused by a disruption in normal brain development because of the presence of gene defects that regulate how brain cells communicate.
Currently, there is no cure for ASD, so traditional treatment focuses on skill-oriented training interventions to teach social and language skills, medications for anxiety, depression or obsessive-compulsive behaviors.
Findings: Effects of Medical Cannabis on Autism Spectrum Disorders
Researchers have found what they believe to be a potential link between autism and cannabinoid receptors, particularly cannabinoid 2 receptors (CB2), within the endocannabinoid system 2,5,7,9. One study found that the cell mutations in the brain that have been previously associated with autism block the action of molecules that act on CB2 receptors. These CB2 receptors are the same ones that the cannabinoids found in cannabis act upon 3. A similar study also found that mice with autistic-like behavioral issues possessed upregulated CB2 receptors 8. Another discovered this same prevalence in the upregulation of CB2, but in human subjects 11. These findings regarding the CB2 receptors support the theory that autism could be caused by a disruption of the brain’s ability to send clear signals and in turn raises the possibility that using cannabinoids found in cannabis can restore communication to allow for proper cell function and communication 3.
There’s also evidence supporting cannabinoids efficacy for treating autism 7,9,10. In one study, an autistic child that was given THC for six months reported significant improvements in hyperactivity, lethargy, irritability, stereotypy and inappropriate speech 6.
In addition, mice with similar behavioral characteristics to autistic humans saw a reduction in depression and were able to remain focused on running on the spinning wheel apparatus after given cannabinoids 8. Another study found that boosting cannabinoids in the brain helps to correct behavioral issues that are related to fragile x syndrome, the most common known genetic cause of autism 4.
Autism spectrum disorder (ASD) is a term used to classify a range of complex neurodevelopment disorders that are characterized, in varying degrees, by social interaction difficulties, verbal and physical communication problems, and restricted and repetitive patterns of behavior. Of the numerous types of ASD’s is autism, also referred to as “classical ASD.” Autism is the most severe form of ASD. Other types of ASD’s include Asperger syndrome, childhood disintegrative disorder, and pervasive developmental disorder-not otherwise specified. According to the National Institute of Neurological Disorders and Stroke, 1 out of 88 children age 8 will have an ASD and males are four times more likely to have one of the disorders than females.
Impaired social interaction is the main sign of ASD and it can become visible as early as infancy. Babies and children with ASD can be unresponsive to people, avoid eye contact or fail to respond to their names. They may focus on one item for a long period of time without noticing any outside stimulation. They struggle at interpreting the thoughts and feelings of others and therefore have problems understanding and responding to social cues like facial expressions and tone of voice. It’s not uncommon for them to lack empathy. Repetitive motions like rocking or twirling, or self-abusive behaviors, like biting or head banging, are common in children with autism.
Very early indicators of an ASD include not responding to one’s name, poor eye contact, no babbling or pointing by age 1, no single words by 16 months, excessive lining up of toys or other objects and no smiling or social responsiveness. Later indicators include an impaired ability to make friends, difficulty initiating or sustaining a conversation, impaired imaginative play, repetitive or unusual language, restricted patterns of focus and the inflexible need to stick with routines.
The causes of ASD are unknown, but according to the National Institute of Neurological Disorders and Stroke, both genetics and environment likely play a role. Brain irregularities and abnormal neurotransmitter levels are commonly found in ASD infants and children, which suggest that the disease is caused by a disruption in normal brain development because of the presence of gene defects that regulate how brain cells communicate.
Currently, there is no cure for ASD, so traditional treatment focuses on skill-oriented training interventions to teach social and language skills, medications for anxiety, depression or obsessive-compulsive behaviors.
Findings: Effects of Medical Cannabis on Autism Spectrum Disorders
Researchers have found what they believe to be a potential link between autism and cannabinoid receptors, particularly cannabinoid 2 receptors (CB2), within the endocannabinoid system 2,5,7,9. One study found that the cell mutations in the brain that have been previously associated with autism block the action of molecules that act on CB2 receptors. These CB2 receptors are the same ones that the cannabinoids found in cannabis act upon 3. A similar study also found that mice with autistic-like behavioral issues possessed upregulated CB2 receptors 8. Another discovered this same prevalence in the upregulation of CB2, but in human subjects 11. These findings regarding the CB2 receptors support the theory that autism could be caused by a disruption of the brain’s ability to send clear signals and in turn raises the possibility that using cannabinoids found in cannabis can restore communication to allow for proper cell function and communication 3.
There’s also evidence supporting cannabinoids efficacy for treating autism 7,9,10. In one study, an autistic child that was given THC for six months reported significant improvements in hyperactivity, lethargy, irritability, stereotypy and inappropriate speech 6.
In addition, mice with similar behavioral characteristics to autistic humans saw a reduction in depression and were able to remain focused on running on the spinning wheel apparatus after given cannabinoids 8. Another study found that boosting cannabinoids in the brain helps to correct behavioral issues that are related to fragile x syndrome, the most common known genetic cause of autism 4.
STATES THAT HAVE APPROVED MEDICAL MEDICAL CANNABIS FOR AUTISM
Minnesota (effective starting in July 2018), Louisiana, and Pennsylvania are the only states to have approved medical cannabis for autism. Colorado is in the process of currently adding ASD into their medical cannabis program too.
A number of other states do, however, consider allowing cannabis for conditions that are not specified in their list of approved conditions. An approval or physician recommendation is required for consideration. These states include: California (any debilitating illness where the medical use of cannabis has been recommended by a physician), Connecticut (other medical conditions may be approved by the Department of Consumer Protection), Massachusetts (other conditions as determined in writing by a qualifying patient’s physician), Nevada (other conditions subject to approval), Oregon (other conditions subject to approval), Rhode Island (other conditions subject to approval), and Washington (any “terminal or debilitating condition”).
In Washington D.C., any condition can be approved for medical cannabis as long as a DC-licensed physician recommends the treatment.
Studies on the Effects of Medical Cannabis on ASD
- An autistic child given THC for six months reported significant reductions in the symptoms of autism. Use of dronabinol (delta-9-THC) in autism: A prospective single-case-study with an early infantile autistic child. (http://www.cannabis-med.org/data/pdf/en_2010_04_1.pdf)
- Mice with similar behavioral characteristics to autistic humans saw an enhanced reduction in depression and were able to remain focused on running on the spinning wheel apparatus. Consequences of cannabinoid and monoaminergic system disruption in a mouse model of autism spectrum disorders. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3137184/).
Autism Fact Sheet. (n.d.). National Institute of Neurological Disorders and Stroke. Retrieved from http://www.ninds.nih.gov/disorders/autism/detail_autism.htm.
Chakrabari, B., and Baron-Cohen, S. (2011). Variation in the human cannabinoid receptor CNR1 gene modulates gaze duration for happy faces. Molecular Autism, 2,10. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3155489/.
Foldy, C., Malenka, R.C., and Sudhof, T.C. (2013, May 8). Autism-associated neuroligin-3 mutations commonly disrupt tonic endocannabinoid signaling. Neuron, 78(3), 498-509. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3663050/.
Jung, K.M., Sepers, M., Henstridge, C.M., Lassalle, O., Neuhofer, D., Martin, H., Ginger, M., Frick, A., DiPatrizio, N.V., Mackie, K., Katona, I., Piomelli, D., and Manzoni, OJ. (2012). Uncoupling of the endocannabinoid signalling complex in a mouse model of fragile x syndrome. Nature Communications, 3:1080. doi: 10.1038/ncomms2045. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3657999/.
Kerr, D.M., Downey, L., Conboy, M., Finn, D.P., and Roche, M. (2013). Alternations in the endocannabinoid system in the rat valproic acid model of autism. Behavioural Brain Research, 249, 124-132. Retrieved from http://www.sciencedirect.com/science/article/pii/S0166432813002519.
Kurz, R., and Blass, K. (2010). Use of dronabinol (delta-9-THC) in autism: A prospective single-case-study with an early infantile autistic child. Cannabinoids, 5(4), 4-6. Retrieved from https://cannabis-med.org/data/pdf/en_2010_04_1.pdf.
Liu, Q.T., Pan, C.H., Hishimoto, A., Li, C.Y., Xi, Z.X., Llorente-Berzal, A., Viveros, M.P., Ishiguro, H., Arinami, T., Onaivi, E.S., and Uhl, G.R. (2009). Species differences in cannabinoid receptor 2 (CNR2 gene): Identification of novel human and rodent CB2 isoforms, differential tissue expression and regulation by cannabinoid receptor ligands. Genes, Brain and Behavior, 8, 519-530. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3389515/.
Onaivi, E.S., Benno, R., Halpern, T., Mehanovic, M., Schanz, N., Sanders, C., Yan, X., Ishiguro, H., Liu, Q.R., Berzal, A.L., Viveros, M.P., and Ali, S.F. (2011, March). Consequences of cannabinoid and monoaminergic system disruption in a mouse model of autism spectrum disorders. Current Neuropharmacology, 9(1), 209-14. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3137184/.
Schneider, M., and Koch, M. (2005). Deficient Social and Play Behavior in Juvenile and Adult Rats after Neonatal Cortical Lesion: Effects of Chronic Pubertal Cannabinoid Treatment. Neuropsychopharmacology, 30, 944-957. Retrieved from http://www.nature.com/npp/journal/v30/n5/full/1300634a.html.
Siniscalo, D. (2014). Endocannabinoid System as Novel Therapeutic Target for Autism Treatment. Autism – Open Access, 4,2, Retrieved from https://www.omicsgroup.org/journals/endocannabinoid-system-as-novel-therapeutic-target-for-autism-treatment-2165-7890.1000e122.pdf.
Siniscalco, D., Sapone, A., Giordano, C., Cirillo, A., de Magistris, L., Rossi, F., Fasano, A., Bradstreet, J.J., Maione, S., and Antonucci, N. (2013, November). Cannabinoid receptor type 2, but not type 1, is up-regulated in peripheral blood mononuclear cells of children affected by autistic disorders. Journal of Autism and Developmental Disorders, 43(11), 2686-95. Retrieved from http://link.springer.com/article/10.1007/s10803-013-1824-9.
What Is Autism? (n.d.). Autism Speaks. Retrieved from https://www.autismspeaks.org/what-autism.
Studies on the Effects of Medical Cannabis on ASD Continued;
Research Part One: The Endocannabinoid System and Autism Spectrum Disorder (ASD)
The importance of the discovery of the role that the endocannabinoid system (ECS) plays in human health and disease cannot be understated. Cannabinoid receptors are the most highly expressed of any G-protein coupled receptor (GPCR) in the body. They’re the only ones to play a direct role in virtually every aspect of the human body (CNS and immune systems, throughout the periphery, presynaptic, and postsynaptic).[1]
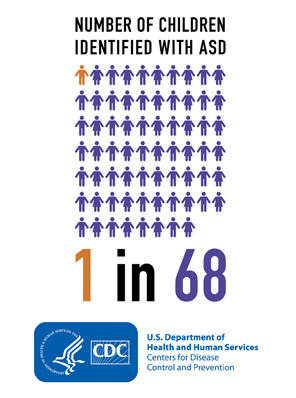
It’s no wonder that anecdotal reports of cannabis treatments indicate effectiveness in such a wide array of conditions. The growing body of scientific research surrounding the endocannabinoid system continues to lead to the further understanding of the physiological basis in a growing number of conditions.[45]
One condition with both supportive anecdotal and preclinical scientific evidence is for patients on the severe end of the autism spectrum (ASD). In a short series of articles we’ll attempt to shed light on the role that the endocannabinoid system plays in the progression of autism, the potential role of phytocannabinoids in treatment, and what that might mean in a practical sense.
NL3 Mutations Inhibit Tonic Endocannabinoid Secretions
Neuroligins are part of a family of neuronal cell surface proteins that “connect presynaptic and postsynaptic neurons at synapses, mediate signaling across the synapse, and shape the properties of neural networks by specifying synaptic functions”. Alterations in genes encoding neuroligins are associated with autism and other cognitive diseases.[56]
Mutations in neuroligin-3 (NL3), a member of the family of neuroligins, are associated with ASD.[17] NL3 is required for tonic secretion of endocannabinoids (AEA, 2-AG).[17] NL3 mutations have been shown to inhibit tonic endocannabinoid secretion.[17] This dysregulation in endocannabinoid signaling may contribute to the pathophysiology of autism.[17, 50, 53] These findings have in part prompted researchers to apply to conduct research with nonhuman primates in order to further elucidate this association.[39]
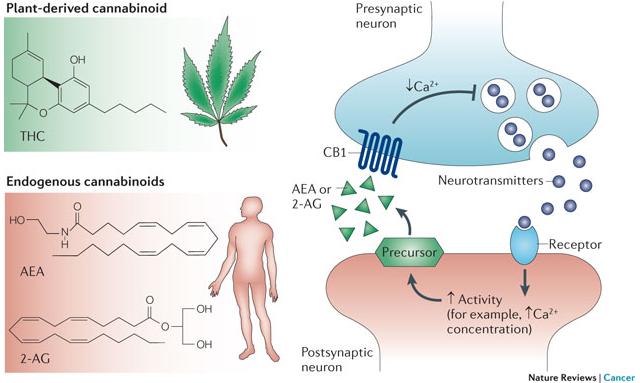
Targeting Endocannabinoid System to Treat FXS
Fragile X syndrome (FXS) is the most commonly known genetic cause of autism.[30] FXS is associated with a loss of the fragile X mental retardation protein (FMRP) which regulates signal transduction in the brain.[30] This FMRP deficiency is believed to “increase neuronal excitability which is mediated by endocannabinoids”.[59]
FXS is also associated with “neuropsychiatric problems such as hyperactivity, attention disorders, and seizures.”[19] The endocannabinoid system is key to modulating functions that are involved with regulating all of these disorders including “synaptic plasticity, cognitive performance, anxiety, nociception and seizure susceptibility.”[19] The endocannabinoid system is specifically implicated in just about all aspects of FXS including “behavioral, synaptic and molecular manifestations.”[19] Preclinical research implicates CB1 and CB2 as pharmacological targets with the potential to reduce cognitive deficits and anxiety in FXS models in rodents.[19, 59]
Increased Expression of CB2 Receptors Associated with ASD
Though it wasn’t long ago that the role that CB2 receptors played in the human brain was believed to be negligible, additional research has implicated it as having a much more substantial role than previously understood.
“Given that CB2 is up-regulated, and that it’s believed to play a neuroprotective role, CB2 is being investigated as a potential target for treatment of ASD.[53]”
One example is that CB2 is believed to play a neuroprotective role in response to a variety of inflammatory stimuli, this has implications in a number of neuropsychiatric conditions including ASD.[4, 16, 53]
In ASD, as well as a number of conditions, the expression level of CB2 receptors increases in response to the inflammatory nature of the condition.[16, 53] Given that CB2 is up-regulated, and that it’s believed to play a neuroprotective role, CB2 is being investigated as a potential target for treatment of ASD.[53]
Elevated Cytokine Levels Associated with ASD
“Cytokines are small secreted proteins released by cells that have a specific effect on the interactions and communications between cells… Pro-inflammatory cytokines are involved in the up-regulation of inflammatory reactions.”[60]
Elevated pro-inflammatory cytokine levels are associated with ASD.[44] Whether this is due in part as a result of NL3 mutations inhibiting tonic secretion of endocannabinoids remains uncertain. However, endocannabinoids (AEA, 2-AG) have been shown to play key roles inhibiting cytokines via CB2.[12, 47]
The majority of cannabinoids have been demonstrated to decrease cytokine production via CB1/CB2 dependent and independent mechanisms.[25, 27, 29, 36]
Clinically Diagnosing ASD via the ECS
A team of researchers recently discovered and patented a process that claims that it’s possible to clinically diagnose ASD, and susceptibility to it, via observation of the degree of modulation that acetaminophen has on endocannabinoid levels. However, based on a series of deductions made within their published literature, it appears that additional research is required.
Other Relevant ECS/ASD Implications
The number of functions that ECS regulate is extensive and beyond the scope of this paper.[45, 48] However, a few potentially relevant aspects to ASD will be listed:
Tonic secretions of endocannabinoids regulate GI functions (including metabolism).[15, 37]
Endocannabinoids regulate stress responses, in part via the modulation of the 5-HT system.[23]
Additional targets of endocannabinoids (and exogenous cannabinoids), PPARα, PPARγ, and GPR55 expression levels have shown reductions in a valproic acid model of autism in rats.[33]
Conclusion
Based on the preclinical research the endocannabinoid system appears to be directly impacted by, as well as a potential target for treatment of, physiological manifestations of genetic factors associated with ASD including NL3 mutations and FXS. NL3 mutations inhibit tonic secretion of endocannabinoids and disrupt their signaling. This possibly contributes to the identified increase in proinflammatory cytokines levels in ASD. CB2 is upregulated in the brain in response to inflammatory stimuli as part of a neuroprotective role, and is suggested as a target for treatment. There appears to be a preponderance of evidence that the ECS is involved in the progression of ASD.
Fragile X syndrome (FXS) is the most commonly known genetic cause of autism.[30] FXS is associated with a loss of the fragile X mental retardation protein (FMRP) which regulates signal transduction in the brain.[30] This FMRP deficiency is believed to “increase neuronal excitability which is mediated by endocannabinoids”.[59]
FXS is also associated with “neuropsychiatric problems such as hyperactivity, attention disorders, and seizures.”[19] The endocannabinoid system is key to modulating functions that are involved with regulating all of these disorders including “synaptic plasticity, cognitive performance, anxiety, nociception and seizure susceptibility.”[19] The endocannabinoid system is specifically implicated in just about all aspects of FXS including “behavioral, synaptic and molecular manifestations.”[19] Preclinical research implicates CB1 and CB2 as pharmacological targets with the potential to reduce cognitive deficits and anxiety in FXS models in rodents.[19, 59]
Increased Expression of CB2 Receptors Associated with ASD
Though it wasn’t long ago that the role that CB2 receptors played in the human brain was believed to be negligible, additional research has implicated it as having a much more substantial role than previously understood.
“Given that CB2 is up-regulated, and that it’s believed to play a neuroprotective role, CB2 is being investigated as a potential target for treatment of ASD.[53]”
One example is that CB2 is believed to play a neuroprotective role in response to a variety of inflammatory stimuli, this has implications in a number of neuropsychiatric conditions including ASD.[4, 16, 53]
In ASD, as well as a number of conditions, the expression level of CB2 receptors increases in response to the inflammatory nature of the condition.[16, 53] Given that CB2 is up-regulated, and that it’s believed to play a neuroprotective role, CB2 is being investigated as a potential target for treatment of ASD.[53]
Elevated Cytokine Levels Associated with ASD
“Cytokines are small secreted proteins released by cells that have a specific effect on the interactions and communications between cells… Pro-inflammatory cytokines are involved in the up-regulation of inflammatory reactions.”[60]
Elevated pro-inflammatory cytokine levels are associated with ASD.[44] Whether this is due in part as a result of NL3 mutations inhibiting tonic secretion of endocannabinoids remains uncertain. However, endocannabinoids (AEA, 2-AG) have been shown to play key roles inhibiting cytokines via CB2.[12, 47]
The majority of cannabinoids have been demonstrated to decrease cytokine production via CB1/CB2 dependent and independent mechanisms.[25, 27, 29, 36]
Clinically Diagnosing ASD via the ECS
A team of researchers recently discovered and patented a process that claims that it’s possible to clinically diagnose ASD, and susceptibility to it, via observation of the degree of modulation that acetaminophen has on endocannabinoid levels. However, based on a series of deductions made within their published literature, it appears that additional research is required.
Other Relevant ECS/ASD Implications
The number of functions that ECS regulate is extensive and beyond the scope of this paper.[45, 48] However, a few potentially relevant aspects to ASD will be listed:
“CB1 variations modulate the striatal function that underlies the perception of signals of social reward, such as happy faces. This suggests that CB1 is a key element in the molecular architecture of perception of certain basic emotions. This may have implications for understanding neurodevelopmental conditions marked by atypical eye contact and facial emotion processing, such as ASC.”[13]“Endocannabinoids are key modulators of synaptic function.”[11]
Tonic secretions of endocannabinoids regulate GI functions (including metabolism).[15, 37]
Endocannabinoids regulate stress responses, in part via the modulation of the 5-HT system.[23]
Additional targets of endocannabinoids (and exogenous cannabinoids), PPARα, PPARγ, and GPR55 expression levels have shown reductions in a valproic acid model of autism in rats.[33]
Conclusion
Based on the preclinical research the endocannabinoid system appears to be directly impacted by, as well as a potential target for treatment of, physiological manifestations of genetic factors associated with ASD including NL3 mutations and FXS. NL3 mutations inhibit tonic secretion of endocannabinoids and disrupt their signaling. This possibly contributes to the identified increase in proinflammatory cytokines levels in ASD. CB2 is upregulated in the brain in response to inflammatory stimuli as part of a neuroprotective role, and is suggested as a target for treatment. There appears to be a preponderance of evidence that the ECS is involved in the progression of ASD.
Citations & References
Alger, Bradley. "Getting High on the Endocannabinoid System." Cerebrum (2013).
Andó, Rómeó D., et al. "The inhibitory action of exo-and endocannabinoids on [3H] GABA release are mediated by both CB1 and CB2 receptors in the mouse hippocampus." Neurochemistry International 60.2 (2012): 145-152.
Aso, Ester, et al. "Lack of CB1 receptor activity impairs serotonergic negative feedback." Journal of neurochemistry 109.3 (2009): 935-944.
Benito, C., et al. "Cannabinoid CB2 receptors in human brain inflammation." British journal of pharmacology 153.2 (2008): 277-285.
Best, Aaron R., and Wade G. Regehr. "Serotonin evokes endocannabinoid release and retrogradely suppresses excitatory synapses." The Journal of Neuroscience 28.25 (2008): 6508-6515.
Bolognini, D., et al. "Cannabidiolic acid prevents vomiting in Suncus murinus and nausea‐induced behaviour in rats by enhancing 5‐HT1A receptor activation." British journal of pharmacology 168.6 (2013): 1456-1470.
Booz, George W. "Cannabidiol as an emergent therapeutic strategy for lessening the impact of inflammation on oxidative stress." Free Radical Biology and Medicine 51.5 (2011): 1054-1061.
Braida, Daniela, et al. "5-HT1A receptors are involved in the anxiolytic effect of ∆9-tetrahydrocannabinol and AM 404, the anandamide transport inhibitor, in Sprague–Dawley rats." European journal of pharmacology 555.2 (2007): 156-163.
Carey, Megan R., et al. "Presynaptic CB1 receptors regulate synaptic plasticity at cerebellar parallel fiber synapses." Journal of neurophysiology 105.2 (2011): 958.
Carley, David W., et al. "Functional role for cannabinoids in respiratory stability during sleep." Sleep 25.4 (2002): 391-398.
Castillo, Pablo E., et al. "Endocannabinoid signaling and synaptic function." Neuron 76.1 (2012): 70-81.
Cencioni, Maria Teresa, et al. "Anandamide suppresses proliferation and cytokine release from primary human T-lymphocytes mainly via CB2 receptors." PLoS One 5.1 (2010): e8688.
Chakrabarti, Bhismadev, and Simon Baron-Cohen. "Variation in the human Cannabinoid Receptor (CNR1) gene modulates gaze duration for happy faces." Molecular autism 2.1 (2011): 10.
Di Filippo, Clara, et al. "Cannabinoid CB2 receptor activation reduces mouse myocardial ischemia-reperfusion injury: involvement of cytokine/chemokines and PMN." Journal of leukocyte biology 75.3 (2004): 453-459.
Di Marzo, V., and F. Piscitelli. "Gut feelings about the endocannabinoid system." Neurogastroenterology & Motility 23.5 (2011): 391-398.
Fernández‐Ruiz, Javier, et al. "Prospects for cannabinoid therapies in basal ganglia disorders." British journal of pharmacology 163.7 (2011): 1365-1378.
Földy, Csaba, Robert C. Malenka, and Thomas C. Südhof. "Autism-associated neuroligin-3 mutations commonly disrupt tonic endocannabinoid signaling." Neuron 78.3 (2013): 498-509.
Gamage, Thomas F., and Aron H. Lichtman. "The endocannabinoid system: role in energy regulation." Pediatric blood & cancer 58.1 (2012): 144-148.
Garcia, Arnau Busquets, et al. “New insights into the molecular pathophysiology of fragile X syndrome and therapeutic perspectives from the animal model”, International Journal of Biochemistry and Cell Biology, 53 (2014) 121-126.
Godlewski, Grzegorz, Manfred Göthert, and Barbara Malinowska. "Cannabinoid receptor‐independent inhibition by cannabinoid agonists of the peripheral 5‐HT3 receptor‐mediated von Bezold–Jarisch reflex." British journal of pharmacology 138.5 (2003): 767-774.
Gomes, Felipe V., Leonardo BM Resstel, and Francisco S. Guimarães. "The anxiolytic-like effects of cannabidiol injected into the bed nucleus of the stria terminalis are mediated by 5-HT1A receptors." Psychopharmacology 213.2-3 (2011): 465-473.
Gong, Jian-Ping, et al. "Cannabinoid CB2 receptors: immunohistochemical localization in rat brain." Brain research 1071.1 (2006): 10-23.
Haj-Dahmane, Samir, and Roh-Yu Shen. "Modulation of the serotonin system by endocannabinoid signaling." Neuropharmacology 61.3 (2011): 414-420.
Iring, András, et al. "Role of Endocannabinoids and Cannabinoid-1 Receptors in Cerebrocortical Blood Flow Regulation." PloS one 8.1 (2013): e53390.
Izzo, Angelo A., et al. "Non-psychotropic plant cannabinoids: new therapeutic opportunities from an ancient herb." Trends in pharmacological sciences 30.10 (2009): 515-527.
Jean-Gilles, Lucie, Bruno Gran, and Cris S. Constantinescu. "Interaction between cytokines, cannabinoids and the nervous system." Immunobiology 215.8 (2010): 606-610.
Jiang, Chengyu, Adrian T. Ting, and Brian Seed. "PPAR-γ agonists inhibit production of monocyte inflammatory cytokines." Nature 391.6662 (1998): 8286.
Johnson, Jeremy R., et al. "Multicenter, double-blind, randomized, placebocontrolled, parallel-group study of the efficacy, safety, and tolerability of THC: CBD extract and THC extract in patients with intractable cancer-related pain." Journal of pain and symptom management 39.2 (2010): 167-179.
Juknat, Ana, et al. "Cannabidiol affects the expression of genes involved in zinc homeostasis in BV-2 microglial cells." Neurochemistry international 61.6 (2012): 923-930.
Jung, Kwang-Mook, et al. "Uncoupling of the endocannabinoid signalling complex in a mouse model of fragile X syndrome." Nature communications 3 (2012): 1080.
Katona, István, and Tamás F. Freund. "Multiple functions of endocannabinoid signaling in the brain." Annual review of neuroscience 35 (2012): 529-558.
Kawamura, Yoshinobu, et al. "The CB1 cannabinoid receptor is the major cannabinoid receptor at excitatory presynaptic sites in the hippocampus and cerebellum." The Journal of neuroscience 26.11 (2006): 2991-3001.
Kerr, D. M., et al. "Alterations in the endocannabinoid system in the rat valproic acid model of autism." Behavioural brain research 249 (2013): 124-132.
Kishimoto, Yasushi, and Masanobu Kano. "Endogenous cannabinoid signaling through the CB1 receptor is essential for cerebellum-dependent discrete motor learning." The Journal of neuroscience 26.34 (2006): 8829-8837.
Klegeris, Andis, Christopher J. Bissonnette, and Patrick L. McGeer. "Reduction of human monocytic cell neurotoxicity and cytokine secretion by ligands of the cannabinoid‐type CB2 receptor." British journal of pharmacology 139.4 (2003): 775-786.
Kozela, Ewa, et al. "Cannabinoids ∆9-tetrahydrocannabinol and cannabidiol differentially inhibit the lipopolysaccharide-activated NF-κB and interferonβ/STAT proinflammatory pathways in BV-2 microglial cells." Journal of biological chemistry 285.3 (2010): 1616-1626.
Li, Chen, Peter M. Jones, and Shanta J. Persaud. "Role of the endocannabinoid system in food intake, energy homeostasis and regulation of the endocrine pancreas." Pharmacology & therapeutics 129.3 (2011): 307-320.
Machado Bergamaschi, Mateus, et al. "Safety and side effects of cannabidiol, a Cannabis sativa constituent." Current drug safety 6.4 (2011): 237-249.
Malcher-Lopes, Renato. "Targeting alterations in the endocannabinoid system of rodents and non-human primates for the study of autism." Qatar Foundation Annual Research Conference. No. 2013. 2013.
Marco, Eva M., et al. "Endocannabinoid system and psychiatry: in search of a neurobiological basis for detrimental and potential therapeutic effects." Frontiers in behavioral neuroscience 5 (2011).
Mato, Susana, et al. "CB1 knockout mice display impaired functionality of 5‐HT1A and 5‐HT2A/C receptors." Journal of neurochemistry 103.5 (2007): 2111-2120.
Mikics, Eva, et al. "Interactions between the anxiogenic effects of CB1 gene disruption and 5-HT3 neurotransmission." Behavioural pharmacology 20.3 (2009): 265-272.
Müller‐Vahl, K. R., et al. "Cannabinoids: possible role in patho‐physiology and therapy of Gilles de la Tourette syndrome." Acta Psychiatrica Scandinavica 98.6 (1998): 502-506.
Napolioni, Valerio, et al. "Plasma cytokine profiling in sibling pairs discordant for autism spectrum disorder." Journal of neuroinflammation 10.1 (2013): 38.
Pacher, Pál, Sándor Bátkai, and George Kunos. "The endocannabinoid system as an emerging target of pharmacotherapy." Pharmacological reviews 58.3 (2006): 389-462.
Palazuelos, Javier, et al. "CB2 cannabinoid receptors promote neural progenitor cell proliferation via mTORC1 signaling." Journal of Biological Chemistry 287.2 (2012): 1198-1209.
Panikashvili, David, et al. "The endocannabinoid 2-AG protects the blood–brain barrier after closed head injury and inhibits mRNA expression of proinflammatory cytokines." Neurobiology of disease 22.2 (2006): 257-264.
Pertwee, R. G., et al. "International Union of Basic and Clinical Pharmacology. LXXIX. Cannabinoid receptors and their ligands: beyond CB1 and CB2." Pharmacological reviews 62.4 (2010): 588-631.
Pomerantz, Daniel J. "THE ROLE OF CB2 ENDOCANNABINOID RECEPTOR AND MTORC1 IN NEUROPROGENITOR CELL PROLIFERATION IN TUBEROUS SCLEROSIS." Emphasis Program (2013): 73.
Onaivi, E. S., et al. "Consequences of cannabinoid and monoaminergic system disruption in a mouse model of autism spectrum disorders." Current neuropharmacology 9.1 (2011): 209.
Rock, Erin. Cannabidiol Indirectly Activates 5-HT1A Somatodendritic Autoreceptors to Attenuate Vomiting and Nausea. Diss. 2011.
Roloff, Alan M., et al. "Homer 1a gates the induction mechanism for endocannabinoid-mediated synaptic plasticity." The Journal of Neuroscience 30.8 (2010): 3072-3081.
Siniscalco, Dario, et al. "Cannabinoid receptor type 2, but not type 1, is upregulated in peripheral blood mononuclear cells of children affected by autistic disorders." Journal of autism and developmental disorders 43.11 (2013): 26862695.
Sharkey, Keith A., Nissar A. Darmani, and Linda A. Parker. "Regulation of nausea and vomiting by cannabinoids and the endocannabinoid system." European journal of pharmacology 722 (2014): 134-146.
Stone, Joe, et al. “Cannabinoids, Ketogenic Diets, Holy Basil, and the PPAR Connection.” Unpublished (2014) http://www.scribd.com/doc/207827158/Cannabinoids-Ketogenic-Diets-HolyBasil-and-the-PPAR-Connection
Sudhof, Thomas C., et al. “Neuroligins and neurexins link synaptic function to cognitive disease”, Nature, 2008/10/16/print, Nature Publishing Group, http://dx.doi.org/10.1038/nature07456
Tanimura, Asami, et al. "Not glutamate but endocannabinoids mediate retrograde suppression of cerebellar parallel fiber to Purkinje cell synaptic transmission in young adult rodents." Neuropharmacology 57.2 (2009): 157-163.
Vaney, C., et al. "Efficacy, safety and tolerability of an orally administered cannabis extract in the treatment of spasticity in patients with multiple sclerosis: a randomized, double-blind, placebo-controlled, crossover study." Multiple Sclerosis 10.4 (2004): 417-424.
Zhang Longhua, Alger Bradley E., et al. “Enhanced Endocannabinoid Signaling Elevates Neuronal Excitability in Fragile X Syndrome” 2010
Zhang, Jun-Ming, and Jianxiong An., et al. “Cytokines, Inflammation and Pain.” International anesthesiology clinics2 (2007): 27–37. PMC. Web. 11 June 2015.
In part one of this series the preclinical scientific evidence illustrating the involvement of the endocannabinoid system (ECS) in the physiological progression of Autism Spectrum Disorder (ASD) was provided. Here we’ll highlight some of the pharmacological characteristics that phytocannabinoids share with endocannabinoids, the use of phytocannabinoids in the treatment of symptoms and diseases associated with ASD, and why having access to a variety of cannabis chemotypes will always be preferable to a select cannabinoid and/or ratio.
The anecdotal reports of successful cannabinoid therapies seem to be supported by the fact that phytocannabinoids from cannabis, and other natural sources, display similar pharmacological characteristics to that of endocannabinoids that are dysregulated in ASD.[31] The potential therapeutic value of supplementing the endocannabinoid system with phytocannabinoids has been suggested in the treatment of a number of diseases with suspected underlying endocannabinoid deficiencies.[34] Documentation of the safety and clinical efficacy of phytocannabinoids in a variety of treatments continues to grow.[16] In regards to the treatment of ASD, some similar characteristics are worth highlighting, including:
Promotion of Neurogenesis[19, 2, 5]
Neuroprotection[15, 23, 35]
Powerful Antioxidants[3, 31, 15]
Neuromodulation[8, 23, 31, 43]
Anti-inflammatory[31, 18]
Based on preclinical research ECS deficiencies appear to be associated with ASD, and it’s implicated as a potential target for treatment. Phytocannabinoids target the ECS and display similar pharmacological characteristics to endocannabinoids that are dysregulated. It’s been suggested that therapies for conditions with corresponding ECS deficiencies may include supplementation with phytocannabinoids. This seems to potentially support the anecdotal reports of successful cannabinoid therapies in ASD.
Treating Symptoms Associated with ASD
There is a considerable body of supportive preclinical data in regards to targeting the ECS with phytocannabinoids in the treatment of a number of symptoms and diseases associated with ASD. For sake of brevity some of these will be highlighted and cited:
G.I. Disorders[4, 10, 42]
Repetitive Behaviors[6, 9, 14]
Seizures[20, 32, 40]
Sleep Dysfunction[28, 41]
Self Injurious Behavior and Tantrums[27, 29, 30]
Tuberous Sclerosis[21, 38, 44]
Cerebral Ischemia[37, 7, 26, 12]
Depression/Anxiety[17, 1, 36]
Cachexia[11, 24]
Again, anecdotal reports of success appear to be supported by an abundance of preclinical research that indicates a potential role for phytocannabinoids in the treatment of symptoms and diseases associated with ASD.
Botanical Extracts > Dronabinol
Due to the relatively common off-label use of Dronabinol (a man-made/synthetic form of THC), for ASD therapy, it seems relevant to point out the substantial data, including clinical studies, suggesting that the combined administration of CBD along with THC (and possibly other cannabinoids/terpenes present in cannabis) exhibit additive and synergistic effects. This is known as the entourage effect and results in greater clinical efficacies when compared to either cannabinoid alone.[25, 18, 34]
The second most prominent cannabinoid in cannabis is cannabidiol (CBD).[13] CBD has been shown to inhibit intoxication, sedation, and tachycardia associated with delta-9-tetrahydrocannabinol (THC).[34] It’s been shown to increase the clinical efficacy of THC, while adding therapeutic value in its own right.[34]
A large portion of the research conducted thus far with ASD and cannabinoids has been with Dronabinol (a synthetic form of THC) alone. Dronabinol has indicated potential for treatment in a single adolescent case study of autism.[22] Does that mean THC along with CBD might offer increased clinical efficacy similar to the way they have been demonstrated to with other conditions?[34] Based on the results of previous research and anecdotal reports this might be the case.
The added benefit of additional cannabinoids (and the added benefit of specifically tailoring ratios) is an important component that sets botanical extracts from cannabis apart from THC or CBD alone. This is why having access to a variety of cannabis chemotypes will always have more potential for therapeutic value than a select cannabinoid, ratio, or cannabis chemotype.
Alger, Bradley. "Getting High on the Endocannabinoid System." Cerebrum (2013).
Andó, Rómeó D., et al. "The inhibitory action of exo-and endocannabinoids on [3H] GABA release are mediated by both CB1 and CB2 receptors in the mouse hippocampus." Neurochemistry International 60.2 (2012): 145-152.
Aso, Ester, et al. "Lack of CB1 receptor activity impairs serotonergic negative feedback." Journal of neurochemistry 109.3 (2009): 935-944.
Benito, C., et al. "Cannabinoid CB2 receptors in human brain inflammation." British journal of pharmacology 153.2 (2008): 277-285.
Best, Aaron R., and Wade G. Regehr. "Serotonin evokes endocannabinoid release and retrogradely suppresses excitatory synapses." The Journal of Neuroscience 28.25 (2008): 6508-6515.
Bolognini, D., et al. "Cannabidiolic acid prevents vomiting in Suncus murinus and nausea‐induced behaviour in rats by enhancing 5‐HT1A receptor activation." British journal of pharmacology 168.6 (2013): 1456-1470.
Booz, George W. "Cannabidiol as an emergent therapeutic strategy for lessening the impact of inflammation on oxidative stress." Free Radical Biology and Medicine 51.5 (2011): 1054-1061.
Braida, Daniela, et al. "5-HT1A receptors are involved in the anxiolytic effect of ∆9-tetrahydrocannabinol and AM 404, the anandamide transport inhibitor, in Sprague–Dawley rats." European journal of pharmacology 555.2 (2007): 156-163.
Carey, Megan R., et al. "Presynaptic CB1 receptors regulate synaptic plasticity at cerebellar parallel fiber synapses." Journal of neurophysiology 105.2 (2011): 958.
Carley, David W., et al. "Functional role for cannabinoids in respiratory stability during sleep." Sleep 25.4 (2002): 391-398.
Castillo, Pablo E., et al. "Endocannabinoid signaling and synaptic function." Neuron 76.1 (2012): 70-81.
Cencioni, Maria Teresa, et al. "Anandamide suppresses proliferation and cytokine release from primary human T-lymphocytes mainly via CB2 receptors." PLoS One 5.1 (2010): e8688.
Chakrabarti, Bhismadev, and Simon Baron-Cohen. "Variation in the human Cannabinoid Receptor (CNR1) gene modulates gaze duration for happy faces." Molecular autism 2.1 (2011): 10.
Di Filippo, Clara, et al. "Cannabinoid CB2 receptor activation reduces mouse myocardial ischemia-reperfusion injury: involvement of cytokine/chemokines and PMN." Journal of leukocyte biology 75.3 (2004): 453-459.
Di Marzo, V., and F. Piscitelli. "Gut feelings about the endocannabinoid system." Neurogastroenterology & Motility 23.5 (2011): 391-398.
Fernández‐Ruiz, Javier, et al. "Prospects for cannabinoid therapies in basal ganglia disorders." British journal of pharmacology 163.7 (2011): 1365-1378.
Földy, Csaba, Robert C. Malenka, and Thomas C. Südhof. "Autism-associated neuroligin-3 mutations commonly disrupt tonic endocannabinoid signaling." Neuron 78.3 (2013): 498-509.
Gamage, Thomas F., and Aron H. Lichtman. "The endocannabinoid system: role in energy regulation." Pediatric blood & cancer 58.1 (2012): 144-148.
Garcia, Arnau Busquets, et al. “New insights into the molecular pathophysiology of fragile X syndrome and therapeutic perspectives from the animal model”, International Journal of Biochemistry and Cell Biology, 53 (2014) 121-126.
Godlewski, Grzegorz, Manfred Göthert, and Barbara Malinowska. "Cannabinoid receptor‐independent inhibition by cannabinoid agonists of the peripheral 5‐HT3 receptor‐mediated von Bezold–Jarisch reflex." British journal of pharmacology 138.5 (2003): 767-774.
Gomes, Felipe V., Leonardo BM Resstel, and Francisco S. Guimarães. "The anxiolytic-like effects of cannabidiol injected into the bed nucleus of the stria terminalis are mediated by 5-HT1A receptors." Psychopharmacology 213.2-3 (2011): 465-473.
Gong, Jian-Ping, et al. "Cannabinoid CB2 receptors: immunohistochemical localization in rat brain." Brain research 1071.1 (2006): 10-23.
Haj-Dahmane, Samir, and Roh-Yu Shen. "Modulation of the serotonin system by endocannabinoid signaling." Neuropharmacology 61.3 (2011): 414-420.
Iring, András, et al. "Role of Endocannabinoids and Cannabinoid-1 Receptors in Cerebrocortical Blood Flow Regulation." PloS one 8.1 (2013): e53390.
Izzo, Angelo A., et al. "Non-psychotropic plant cannabinoids: new therapeutic opportunities from an ancient herb." Trends in pharmacological sciences 30.10 (2009): 515-527.
Jean-Gilles, Lucie, Bruno Gran, and Cris S. Constantinescu. "Interaction between cytokines, cannabinoids and the nervous system." Immunobiology 215.8 (2010): 606-610.
Jiang, Chengyu, Adrian T. Ting, and Brian Seed. "PPAR-γ agonists inhibit production of monocyte inflammatory cytokines." Nature 391.6662 (1998): 8286.
Johnson, Jeremy R., et al. "Multicenter, double-blind, randomized, placebocontrolled, parallel-group study of the efficacy, safety, and tolerability of THC: CBD extract and THC extract in patients with intractable cancer-related pain." Journal of pain and symptom management 39.2 (2010): 167-179.
Juknat, Ana, et al. "Cannabidiol affects the expression of genes involved in zinc homeostasis in BV-2 microglial cells." Neurochemistry international 61.6 (2012): 923-930.
Jung, Kwang-Mook, et al. "Uncoupling of the endocannabinoid signalling complex in a mouse model of fragile X syndrome." Nature communications 3 (2012): 1080.
Katona, István, and Tamás F. Freund. "Multiple functions of endocannabinoid signaling in the brain." Annual review of neuroscience 35 (2012): 529-558.
Kawamura, Yoshinobu, et al. "The CB1 cannabinoid receptor is the major cannabinoid receptor at excitatory presynaptic sites in the hippocampus and cerebellum." The Journal of neuroscience 26.11 (2006): 2991-3001.
Kerr, D. M., et al. "Alterations in the endocannabinoid system in the rat valproic acid model of autism." Behavioural brain research 249 (2013): 124-132.
Kishimoto, Yasushi, and Masanobu Kano. "Endogenous cannabinoid signaling through the CB1 receptor is essential for cerebellum-dependent discrete motor learning." The Journal of neuroscience 26.34 (2006): 8829-8837.
Klegeris, Andis, Christopher J. Bissonnette, and Patrick L. McGeer. "Reduction of human monocytic cell neurotoxicity and cytokine secretion by ligands of the cannabinoid‐type CB2 receptor." British journal of pharmacology 139.4 (2003): 775-786.
Kozela, Ewa, et al. "Cannabinoids ∆9-tetrahydrocannabinol and cannabidiol differentially inhibit the lipopolysaccharide-activated NF-κB and interferonβ/STAT proinflammatory pathways in BV-2 microglial cells." Journal of biological chemistry 285.3 (2010): 1616-1626.
Li, Chen, Peter M. Jones, and Shanta J. Persaud. "Role of the endocannabinoid system in food intake, energy homeostasis and regulation of the endocrine pancreas." Pharmacology & therapeutics 129.3 (2011): 307-320.
Machado Bergamaschi, Mateus, et al. "Safety and side effects of cannabidiol, a Cannabis sativa constituent." Current drug safety 6.4 (2011): 237-249.
Malcher-Lopes, Renato. "Targeting alterations in the endocannabinoid system of rodents and non-human primates for the study of autism." Qatar Foundation Annual Research Conference. No. 2013. 2013.
Marco, Eva M., et al. "Endocannabinoid system and psychiatry: in search of a neurobiological basis for detrimental and potential therapeutic effects." Frontiers in behavioral neuroscience 5 (2011).
Mato, Susana, et al. "CB1 knockout mice display impaired functionality of 5‐HT1A and 5‐HT2A/C receptors." Journal of neurochemistry 103.5 (2007): 2111-2120.
Mikics, Eva, et al. "Interactions between the anxiogenic effects of CB1 gene disruption and 5-HT3 neurotransmission." Behavioural pharmacology 20.3 (2009): 265-272.
Müller‐Vahl, K. R., et al. "Cannabinoids: possible role in patho‐physiology and therapy of Gilles de la Tourette syndrome." Acta Psychiatrica Scandinavica 98.6 (1998): 502-506.
Napolioni, Valerio, et al. "Plasma cytokine profiling in sibling pairs discordant for autism spectrum disorder." Journal of neuroinflammation 10.1 (2013): 38.
Pacher, Pál, Sándor Bátkai, and George Kunos. "The endocannabinoid system as an emerging target of pharmacotherapy." Pharmacological reviews 58.3 (2006): 389-462.
Palazuelos, Javier, et al. "CB2 cannabinoid receptors promote neural progenitor cell proliferation via mTORC1 signaling." Journal of Biological Chemistry 287.2 (2012): 1198-1209.
Panikashvili, David, et al. "The endocannabinoid 2-AG protects the blood–brain barrier after closed head injury and inhibits mRNA expression of proinflammatory cytokines." Neurobiology of disease 22.2 (2006): 257-264.
Pertwee, R. G., et al. "International Union of Basic and Clinical Pharmacology. LXXIX. Cannabinoid receptors and their ligands: beyond CB1 and CB2." Pharmacological reviews 62.4 (2010): 588-631.
Pomerantz, Daniel J. "THE ROLE OF CB2 ENDOCANNABINOID RECEPTOR AND MTORC1 IN NEUROPROGENITOR CELL PROLIFERATION IN TUBEROUS SCLEROSIS." Emphasis Program (2013): 73.
Onaivi, E. S., et al. "Consequences of cannabinoid and monoaminergic system disruption in a mouse model of autism spectrum disorders." Current neuropharmacology 9.1 (2011): 209.
Rock, Erin. Cannabidiol Indirectly Activates 5-HT1A Somatodendritic Autoreceptors to Attenuate Vomiting and Nausea. Diss. 2011.
Roloff, Alan M., et al. "Homer 1a gates the induction mechanism for endocannabinoid-mediated synaptic plasticity." The Journal of Neuroscience 30.8 (2010): 3072-3081.
Siniscalco, Dario, et al. "Cannabinoid receptor type 2, but not type 1, is upregulated in peripheral blood mononuclear cells of children affected by autistic disorders." Journal of autism and developmental disorders 43.11 (2013): 26862695.
Sharkey, Keith A., Nissar A. Darmani, and Linda A. Parker. "Regulation of nausea and vomiting by cannabinoids and the endocannabinoid system." European journal of pharmacology 722 (2014): 134-146.
Stone, Joe, et al. “Cannabinoids, Ketogenic Diets, Holy Basil, and the PPAR Connection.” Unpublished (2014) http://www.scribd.com/doc/207827158/Cannabinoids-Ketogenic-Diets-HolyBasil-and-the-PPAR-Connection
Sudhof, Thomas C., et al. “Neuroligins and neurexins link synaptic function to cognitive disease”, Nature, 2008/10/16/print, Nature Publishing Group, http://dx.doi.org/10.1038/nature07456
Tanimura, Asami, et al. "Not glutamate but endocannabinoids mediate retrograde suppression of cerebellar parallel fiber to Purkinje cell synaptic transmission in young adult rodents." Neuropharmacology 57.2 (2009): 157-163.
Vaney, C., et al. "Efficacy, safety and tolerability of an orally administered cannabis extract in the treatment of spasticity in patients with multiple sclerosis: a randomized, double-blind, placebo-controlled, crossover study." Multiple Sclerosis 10.4 (2004): 417-424.
Zhang Longhua, Alger Bradley E., et al. “Enhanced Endocannabinoid Signaling Elevates Neuronal Excitability in Fragile X Syndrome” 2010
Zhang, Jun-Ming, and Jianxiong An., et al. “Cytokines, Inflammation and Pain.” International anesthesiology clinics2 (2007): 27–37. PMC. Web. 11 June 2015.
Part Two: The Role of Phytocannabinoids in ASD Therapy
The anecdotal reports of successful cannabinoid therapies seem to be supported by the fact that phytocannabinoids from cannabis, and other natural sources, display similar pharmacological characteristics to that of endocannabinoids that are dysregulated in ASD.[31] The potential therapeutic value of supplementing the endocannabinoid system with phytocannabinoids has been suggested in the treatment of a number of diseases with suspected underlying endocannabinoid deficiencies.[34] Documentation of the safety and clinical efficacy of phytocannabinoids in a variety of treatments continues to grow.[16] In regards to the treatment of ASD, some similar characteristics are worth highlighting, including:
Promotion of Neurogenesis[19, 2, 5]
Neuroprotection[15, 23, 35]
Powerful Antioxidants[3, 31, 15]
Neuromodulation[8, 23, 31, 43]
Anti-inflammatory[31, 18]
Based on preclinical research ECS deficiencies appear to be associated with ASD, and it’s implicated as a potential target for treatment. Phytocannabinoids target the ECS and display similar pharmacological characteristics to endocannabinoids that are dysregulated. It’s been suggested that therapies for conditions with corresponding ECS deficiencies may include supplementation with phytocannabinoids. This seems to potentially support the anecdotal reports of successful cannabinoid therapies in ASD.
Treating Symptoms Associated with ASD
There is a considerable body of supportive preclinical data in regards to targeting the ECS with phytocannabinoids in the treatment of a number of symptoms and diseases associated with ASD. For sake of brevity some of these will be highlighted and cited:
G.I. Disorders[4, 10, 42]
Repetitive Behaviors[6, 9, 14]
Seizures[20, 32, 40]
Sleep Dysfunction[28, 41]
Self Injurious Behavior and Tantrums[27, 29, 30]
Tuberous Sclerosis[21, 38, 44]
Cerebral Ischemia[37, 7, 26, 12]
Depression/Anxiety[17, 1, 36]
Cachexia[11, 24]
Again, anecdotal reports of success appear to be supported by an abundance of preclinical research that indicates a potential role for phytocannabinoids in the treatment of symptoms and diseases associated with ASD.
Botanical Extracts > Dronabinol
Due to the relatively common off-label use of Dronabinol (a man-made/synthetic form of THC), for ASD therapy, it seems relevant to point out the substantial data, including clinical studies, suggesting that the combined administration of CBD along with THC (and possibly other cannabinoids/terpenes present in cannabis) exhibit additive and synergistic effects. This is known as the entourage effect and results in greater clinical efficacies when compared to either cannabinoid alone.[25, 18, 34]
The second most prominent cannabinoid in cannabis is cannabidiol (CBD).[13] CBD has been shown to inhibit intoxication, sedation, and tachycardia associated with delta-9-tetrahydrocannabinol (THC).[34] It’s been shown to increase the clinical efficacy of THC, while adding therapeutic value in its own right.[34]
A large portion of the research conducted thus far with ASD and cannabinoids has been with Dronabinol (a synthetic form of THC) alone. Dronabinol has indicated potential for treatment in a single adolescent case study of autism.[22] Does that mean THC along with CBD might offer increased clinical efficacy similar to the way they have been demonstrated to with other conditions?[34] Based on the results of previous research and anecdotal reports this might be the case.
The added benefit of additional cannabinoids (and the added benefit of specifically tailoring ratios) is an important component that sets botanical extracts from cannabis apart from THC or CBD alone. This is why having access to a variety of cannabis chemotypes will always have more potential for therapeutic value than a select cannabinoid, ratio, or cannabis chemotype.
Discussion
Based on their ability to target the ECS, and their shared characteristics with dysfunctional endocannabinoid levels, preclinical evidence supports the potential therapeutic value of phytocannabinoids in ASD therapy.
Highlighting individual pharmacological characteristics of CBD, THC, and other phytocannabinoids is beyond the scope of this paper. However, based on the ECS deficiencies associated with ASD, and the ability of phytocannabinoids to target and modulate aspects of the deficiencies, anecdotal reports seem to be supported by the best available scientific data. It appears that phytocannabinoids have the potential for therapeutic value in some severe cases of ASD.
Citations & References
Almeida, Valeria, et al. "Cannabidiol exhibits anxiolytic but not antipsychotic property evaluated in the social interaction test." Progress in NeuroPsychopharmacology and Biological Psychiatry 41 (2013): 30-35.
Avraham, Hava Karsenty, et al. "The cannabinoid CB2 receptor agonist AM1241 enhances neurogenesis in GFAP/Gp120 transgenic mice displaying deficits in neurogenesis." British journal of pharmacology2 (2014): 468-479.
Borges, Rosivaldo S., et al. "Understanding the molecular aspects of tetrahydrocannabinol and cannabidiol as antioxidants." Molecules10 (2013): 12663-12674.
Camilleri, Michael, et al. "Cannabinoid receptor 1 gene and irritable bowel syndrome: phenotype and quantitative traits." American Journal of Physiology Gastrointestinal and Liver Physiology 304.5 (2013): G553-G560.
Campos, Alline Cristina, et al. "Multiple mechanisms involved in the largespectrum therapeutic potential of cannabidiol in psychiatric disorders." Philosophical Transactions of the Royal Society B: Biological Sciences 367.1607 (2012): 3364-3378.
Casarotto, Plinio C., et al. "Cannabidiol inhibitory effect on marble-burying behaviour: involvement of CB1 receptors." Behavioural pharmacology 21.4 (2010): 353-358.
Choi, In-Young, et al. "Activation of Cannabinoid CB2 Receptor–Mediated AMPK/CREB Pathway Reduces Cerebral Ischemic Injury." The American journal of pathology 182.3 (2013): 928-939.
Davis, Mellar, et al. "The emerging role of cannabinoid neuromodulators in symptom management." Supportive care in cancer 1 (2007): 63-71.
Deiana, Serena, et al. "Plasma and brain pharmacokinetic profile of cannabidiol (CBD), cannabidivarine (CBDV), ∆9-tetrahydrocannabivarin (THCV) and cannabigerol (CBG) in rats and mice following oral and intraperitoneal administration and CBD action on obsessive–compulsive behaviour." Psychopharmacology 219.3 (2012): 859-873.
Di Sabatino, A., et al. "The endogenous cannabinoid system in the gut of patients with inflammatory bowel disease." Mucosal immunology 4.5 (2011): 574-583.
Engeli, Stefan. "Central and peripheral cannabinoid receptors as therapeutic targets in the control of food intake and body weight." Appetite Control. Springer Berlin Heidelberg, 2012. 357-381.
Garcia-Bonilla, Lidia, et al. "Immune mechanisms in cerebral ischemic tolerance." Frontiers in neuroscience 8 (2014).
Gertsch, Jürg, Roger G. Pertwee, and Vincenzo Di Marzo. "Phytocannabinoids beyond the Cannabis plant–do they exist?." British journal of pharmacology 160.3 (2010): 523-529.
Gomes, Felipe V., et al. "Facilitation of CB1 receptor-mediated neurotransmission decreases marble burying behavior in mice." Progress in NeuroPsychopharmacology and Biological Psychiatry 35.2 (2011): 434-438.
Hampson, Aidan J., Julius Axelrod, and Maurizio Grimaldi. "Cannabinoids as antioxidants and neuroprotectants." U.S. Patent No. 6,630,507. 7 Oct. 2003.
Hazekamp, Arno, and Franjo Grotenhermen. "Clinical Studies With Cannabis and Cannabinoids, 2005-2009." (2013).
Hill, Matthew N., and Boris B. Gorzalka. "The endocannabinoid system and the treatment of mood and anxiety disorders." CNS & Neurological Disorders-Drug Targets (Formerly Current Drug Targets-CNS & Neurological Disorders) 8.6 (2009): 451-458.
Izzo, Angelo A., et al. "Non-psychotropic plant cannabinoids: new therapeutic opportunities from an ancient herb." Trends in pharmacological sciences 30.10 (2009): 515-527.
Jiang, Wen, et al. "Cannabinoids promote embryonic and adult hippocampus neurogenesis and produce anxiolytic-and antidepressant-like effects." Journal of Clinical Investigation11 (2005): 3104.
Jones, Nicholas A., et al. "Cannabidiol exerts anti-convulsant effects in animal models of temporal lobe and partial seizures." Seizure 21.5 (2012): 344-352.
Krueger, Dilja D., and Nils Brose. "Evidence for a common endocannabinoidrelated pathomechanism in autism spectrum disorders." Neuron 78.3 (2013): 408410.
Kurz, René, and Kurt Blaas. "Use of dronabinol (delta-9-THC) in autism: A prospective single-case-study with an early infantile autistic child." (2010)
Lara-Celador, I. et al. “Using the Endocannabinoid System as a Neuroprotective Strategy in Perinatal Hypoxic-Ischemic Brain Injury.” Neural Regeneration Research8 (2013): 731–744.
Marco, Eva M., et al. "The role of the endocannabinoid system in eating disorders: pharmacological implications." Behavioural pharmacology 23.5 and 6 (2012): 526-536.
McPartland, John M., and Ethan B. Russo. "Cannabis and cannabis extracts: greater than the sum of their parts?." Journal of Cannabis Therapeutics 1.3-4 (2001): 103-132.
Murikinati, Sasidhar, et al. "Activation of cannabinoid 2 receptors protects against cerebral ischemia by inhibiting neutrophil recruitment." The FASEB journal 24.3 (2010): 788-798.
Müller-Vahl, K. R., et al. "Cannabis in movement disorders." Forschende Komplementärmedizin/Research in Complementary Medicine 6.Suppl. 3 (2004): 23-27.
Murillo-Rodriguez, Eric, et al. "The emerging role of the endocannabinoid system in the sleep-wake cycle modulation." Central Nervous System Agents in Medicinal Chemistry (Formerly Current Medicinal Chemistry-Central Nervous System Agents) 11.3 (2011): 189-196.
Onaivi, E. S., et al. "Consequences of cannabinoid and monoaminergic system disruption in a mouse model of autism spectrum disorders." Current neuropharmacology 9.1 (2011): 209.
Passie, Torsten, et al. "Mitigation of post‐traumatic stress symptoms by Cannabis resin: A review of the clinical and neurobiological evidence." Drug testing and analysis7-8 (2012): 649-659.
Pertwee, R. G., et al. "International Union of Basic and Clinical Pharmacology. LXXIX. Cannabinoid receptors and their ligands: beyond CB1 and CB2." Pharmacological reviews 62.4 (2010): 588-631.
Porter, Brenda E., and Catherine Jacobson. "Report of a parent survey of cannabidiol-enriched cannabis use in pediatric treatment-resistant epilepsy." Epilepsy & Behavior 29.3 (2013): 574-577.
Russo, Ethan, and Geoffrey W. Guy. "A tale of two cannabinoids: the therapeutic rationale for combining tetrahydrocannabinol and cannabidiol." Medical hypotheses 66.2 (2006): 234-246.
Russo, Ethan B. "Taming THC: potential cannabis synergy and phytocannabinoid‐terpenoid entourage effects." British Journal of Pharmacology 163.7 (2011): 1344-1364.
Sanchez, A. J., and A. Garcia-Merino. "Neuroprotective agents: cannabinoids." Clinical Immunology1 (2012): 57-67.
Schier, Alexandre Rafael de Mello, et al. "Cannabidiol, a Cannabis sativa constituent, as an anxiolytic drug." Revista Brasileira de Psiquiatria 34 (2012): 104-110.
Schmidt, W., et al. "Cannabinoid receptor subtypes 1 and 2 mediate long-lasting neuroprotection and improve motor behavior deficits after transient focal cerebral ischemia." Neuroscience 227 (2012): 313-326.
Shu, Hai-Feng, et al. "Expression of TRPV1 in cortical lesions from patients with tuberous sclerosis complex and focal cortical dysplasia type IIb." Brain and Development 35.3 (2013): 252-260.
Russo, Ethan B. "Clinical endocannabinoid deficiency (CECD): can this concept explain therapeutic benefits of cannabis in migraine, fibromyalgia, irritable bowel syndrome and other treatment-resistant conditions?." Neuro endocrinology letters 25.1-2 (2003): 31-39.
van Rijn, Clementina M., et al. "Endocannabinoid system protects against cryptogenic seizures." Pharmacol Rep 63 (2011): 165-168.
Ware, Mark A., et al. "The effects of nabilone on sleep in fibromyalgia: results of a randomized controlled trial." Anesthesia & Analgesia 110.2 (2010): 604-610.
Wright, K. L., M. Duncan, and K. A. Sharkey. "Cannabinoid CB2 receptors in the gastrointestinal tract: a regulatory system in states of inflammation." British journal of pharmacology 153.2 (2008): 263-270
Youssef, F. F., and A. J. Irving. "From cannabis to the endocannabinoid system: refocussing attention on potential clinical benefits." West Indian Medical Journal 61.3 (2012).
Zurolo, E., et al. "CB1 and CB2 cannabinoid receptor expression during development and in epileptogenic developmental pathologies." Neuroscience 170.1 (2010): 28-41
In our previous installment, we provided a brief overview of the preclinical research implicating the role that the endocannabinoid system (ECS) plays in the progression of autism spectrum disorder (ASD), preclinical research supporting targeting the ECS to treat ASD, and provided a number of preclinical studies indicating the potential value of phytocannabinoids in treating symptoms and diseases associated with ASD.
Here we’ll examine the shortcomings of current research, explore possible adverse effects of cannabinoid treatments, discuss the types of autism that may currently warrant cannabinoid treatments, and illustrate how a family might systematically approach a cannabinoid treatment for ASD.
Based on their ability to target the ECS, and their shared characteristics with dysfunctional endocannabinoid levels, preclinical evidence supports the potential therapeutic value of phytocannabinoids in ASD therapy.
Highlighting individual pharmacological characteristics of CBD, THC, and other phytocannabinoids is beyond the scope of this paper. However, based on the ECS deficiencies associated with ASD, and the ability of phytocannabinoids to target and modulate aspects of the deficiencies, anecdotal reports seem to be supported by the best available scientific data. It appears that phytocannabinoids have the potential for therapeutic value in some severe cases of ASD.
Citations & References
Almeida, Valeria, et al. "Cannabidiol exhibits anxiolytic but not antipsychotic property evaluated in the social interaction test." Progress in NeuroPsychopharmacology and Biological Psychiatry 41 (2013): 30-35.
Avraham, Hava Karsenty, et al. "The cannabinoid CB2 receptor agonist AM1241 enhances neurogenesis in GFAP/Gp120 transgenic mice displaying deficits in neurogenesis." British journal of pharmacology2 (2014): 468-479.
Borges, Rosivaldo S., et al. "Understanding the molecular aspects of tetrahydrocannabinol and cannabidiol as antioxidants." Molecules10 (2013): 12663-12674.
Camilleri, Michael, et al. "Cannabinoid receptor 1 gene and irritable bowel syndrome: phenotype and quantitative traits." American Journal of Physiology Gastrointestinal and Liver Physiology 304.5 (2013): G553-G560.
Campos, Alline Cristina, et al. "Multiple mechanisms involved in the largespectrum therapeutic potential of cannabidiol in psychiatric disorders." Philosophical Transactions of the Royal Society B: Biological Sciences 367.1607 (2012): 3364-3378.
Casarotto, Plinio C., et al. "Cannabidiol inhibitory effect on marble-burying behaviour: involvement of CB1 receptors." Behavioural pharmacology 21.4 (2010): 353-358.
Choi, In-Young, et al. "Activation of Cannabinoid CB2 Receptor–Mediated AMPK/CREB Pathway Reduces Cerebral Ischemic Injury." The American journal of pathology 182.3 (2013): 928-939.
Davis, Mellar, et al. "The emerging role of cannabinoid neuromodulators in symptom management." Supportive care in cancer 1 (2007): 63-71.
Deiana, Serena, et al. "Plasma and brain pharmacokinetic profile of cannabidiol (CBD), cannabidivarine (CBDV), ∆9-tetrahydrocannabivarin (THCV) and cannabigerol (CBG) in rats and mice following oral and intraperitoneal administration and CBD action on obsessive–compulsive behaviour." Psychopharmacology 219.3 (2012): 859-873.
Di Sabatino, A., et al. "The endogenous cannabinoid system in the gut of patients with inflammatory bowel disease." Mucosal immunology 4.5 (2011): 574-583.
Engeli, Stefan. "Central and peripheral cannabinoid receptors as therapeutic targets in the control of food intake and body weight." Appetite Control. Springer Berlin Heidelberg, 2012. 357-381.
Garcia-Bonilla, Lidia, et al. "Immune mechanisms in cerebral ischemic tolerance." Frontiers in neuroscience 8 (2014).
Gertsch, Jürg, Roger G. Pertwee, and Vincenzo Di Marzo. "Phytocannabinoids beyond the Cannabis plant–do they exist?." British journal of pharmacology 160.3 (2010): 523-529.
Gomes, Felipe V., et al. "Facilitation of CB1 receptor-mediated neurotransmission decreases marble burying behavior in mice." Progress in NeuroPsychopharmacology and Biological Psychiatry 35.2 (2011): 434-438.
Hampson, Aidan J., Julius Axelrod, and Maurizio Grimaldi. "Cannabinoids as antioxidants and neuroprotectants." U.S. Patent No. 6,630,507. 7 Oct. 2003.
Hazekamp, Arno, and Franjo Grotenhermen. "Clinical Studies With Cannabis and Cannabinoids, 2005-2009." (2013).
Hill, Matthew N., and Boris B. Gorzalka. "The endocannabinoid system and the treatment of mood and anxiety disorders." CNS & Neurological Disorders-Drug Targets (Formerly Current Drug Targets-CNS & Neurological Disorders) 8.6 (2009): 451-458.
Izzo, Angelo A., et al. "Non-psychotropic plant cannabinoids: new therapeutic opportunities from an ancient herb." Trends in pharmacological sciences 30.10 (2009): 515-527.
Jiang, Wen, et al. "Cannabinoids promote embryonic and adult hippocampus neurogenesis and produce anxiolytic-and antidepressant-like effects." Journal of Clinical Investigation11 (2005): 3104.
Jones, Nicholas A., et al. "Cannabidiol exerts anti-convulsant effects in animal models of temporal lobe and partial seizures." Seizure 21.5 (2012): 344-352.
Krueger, Dilja D., and Nils Brose. "Evidence for a common endocannabinoidrelated pathomechanism in autism spectrum disorders." Neuron 78.3 (2013): 408410.
Kurz, René, and Kurt Blaas. "Use of dronabinol (delta-9-THC) in autism: A prospective single-case-study with an early infantile autistic child." (2010)
Lara-Celador, I. et al. “Using the Endocannabinoid System as a Neuroprotective Strategy in Perinatal Hypoxic-Ischemic Brain Injury.” Neural Regeneration Research8 (2013): 731–744.
Marco, Eva M., et al. "The role of the endocannabinoid system in eating disorders: pharmacological implications." Behavioural pharmacology 23.5 and 6 (2012): 526-536.
McPartland, John M., and Ethan B. Russo. "Cannabis and cannabis extracts: greater than the sum of their parts?." Journal of Cannabis Therapeutics 1.3-4 (2001): 103-132.
Murikinati, Sasidhar, et al. "Activation of cannabinoid 2 receptors protects against cerebral ischemia by inhibiting neutrophil recruitment." The FASEB journal 24.3 (2010): 788-798.
Müller-Vahl, K. R., et al. "Cannabis in movement disorders." Forschende Komplementärmedizin/Research in Complementary Medicine 6.Suppl. 3 (2004): 23-27.
Murillo-Rodriguez, Eric, et al. "The emerging role of the endocannabinoid system in the sleep-wake cycle modulation." Central Nervous System Agents in Medicinal Chemistry (Formerly Current Medicinal Chemistry-Central Nervous System Agents) 11.3 (2011): 189-196.
Onaivi, E. S., et al. "Consequences of cannabinoid and monoaminergic system disruption in a mouse model of autism spectrum disorders." Current neuropharmacology 9.1 (2011): 209.
Passie, Torsten, et al. "Mitigation of post‐traumatic stress symptoms by Cannabis resin: A review of the clinical and neurobiological evidence." Drug testing and analysis7-8 (2012): 649-659.
Pertwee, R. G., et al. "International Union of Basic and Clinical Pharmacology. LXXIX. Cannabinoid receptors and their ligands: beyond CB1 and CB2." Pharmacological reviews 62.4 (2010): 588-631.
Porter, Brenda E., and Catherine Jacobson. "Report of a parent survey of cannabidiol-enriched cannabis use in pediatric treatment-resistant epilepsy." Epilepsy & Behavior 29.3 (2013): 574-577.
Russo, Ethan, and Geoffrey W. Guy. "A tale of two cannabinoids: the therapeutic rationale for combining tetrahydrocannabinol and cannabidiol." Medical hypotheses 66.2 (2006): 234-246.
Russo, Ethan B. "Taming THC: potential cannabis synergy and phytocannabinoid‐terpenoid entourage effects." British Journal of Pharmacology 163.7 (2011): 1344-1364.
Sanchez, A. J., and A. Garcia-Merino. "Neuroprotective agents: cannabinoids." Clinical Immunology1 (2012): 57-67.
Schier, Alexandre Rafael de Mello, et al. "Cannabidiol, a Cannabis sativa constituent, as an anxiolytic drug." Revista Brasileira de Psiquiatria 34 (2012): 104-110.
Schmidt, W., et al. "Cannabinoid receptor subtypes 1 and 2 mediate long-lasting neuroprotection and improve motor behavior deficits after transient focal cerebral ischemia." Neuroscience 227 (2012): 313-326.
Shu, Hai-Feng, et al. "Expression of TRPV1 in cortical lesions from patients with tuberous sclerosis complex and focal cortical dysplasia type IIb." Brain and Development 35.3 (2013): 252-260.
Russo, Ethan B. "Clinical endocannabinoid deficiency (CECD): can this concept explain therapeutic benefits of cannabis in migraine, fibromyalgia, irritable bowel syndrome and other treatment-resistant conditions?." Neuro endocrinology letters 25.1-2 (2003): 31-39.
van Rijn, Clementina M., et al. "Endocannabinoid system protects against cryptogenic seizures." Pharmacol Rep 63 (2011): 165-168.
Ware, Mark A., et al. "The effects of nabilone on sleep in fibromyalgia: results of a randomized controlled trial." Anesthesia & Analgesia 110.2 (2010): 604-610.
Wright, K. L., M. Duncan, and K. A. Sharkey. "Cannabinoid CB2 receptors in the gastrointestinal tract: a regulatory system in states of inflammation." British journal of pharmacology 153.2 (2008): 263-270
Youssef, F. F., and A. J. Irving. "From cannabis to the endocannabinoid system: refocussing attention on potential clinical benefits." West Indian Medical Journal 61.3 (2012).
Zurolo, E., et al. "CB1 and CB2 cannabinoid receptor expression during development and in epileptogenic developmental pathologies." Neuroscience 170.1 (2010): 28-41
Part Three: Practical Approach to Cannabis Based ASD Therapies
In our previous installment, we provided a brief overview of the preclinical research implicating the role that the endocannabinoid system (ECS) plays in the progression of autism spectrum disorder (ASD), preclinical research supporting targeting the ECS to treat ASD, and provided a number of preclinical studies indicating the potential value of phytocannabinoids in treating symptoms and diseases associated with ASD.
Here we’ll examine the shortcomings of current research, explore possible adverse effects of cannabinoid treatments, discuss the types of autism that may currently warrant cannabinoid treatments, and illustrate how a family might systematically approach a cannabinoid treatment for ASD.
Cannabis Therapy Uncertainties
While the preclinical research appears promising, it’s important to note that preclinical research doesn’t always translate into clinical efficacy; although, anecdotal reports of success do lend themselves to the idea of promise. Additionally, treatments are made more complex by the wide spectrum of ASD and the genetic conditions associated with it.[1, 2] Specific cannabinoids and ratios of cannabinoids (as well as terpenes and flavonoids) that offer the most therapeutic value may vary on an individual case by case basis.
Preclinical research does not yet provide clear cut answers in regards to how to target the endocannabinoid system to treat ASD. CB1 and CB2 blockade decreased cognitive deficits and anxiety, respectively, in some FXS models.[2, 10] Other models indicate the beneficial aspect of combating neuroinflammation via CB2 activation.[9, 5] Many of the symptoms associated with ASD are treated via CB1 activation as cited in the previous article of this installment. The NL3 models indicate a benefit from increasing endocannabinoid levels.[1] NL3 mutations and FXS both have a wide spectrum of dysfunction, the degree of which is different in every patient. [1, 2] Therefore, each patient may display varying ECS dysfunctions and, in turn, require varying ratios of cannabinoids for therapy. This is why it may be important to have access to a selection of cannabis varieties with known ratios of cannabinoids present (primarily CBD:THC).
Possible Adverse Effects
When considering a cannabis treatment for an underage patient and/or a developing brain there may be adverse effects from cannabis treatments that should be considered. Acute and chronic administration of delta-9-tetrahydrocannabinol (THC) has been demonstrated to cause mild cognitive deficits related to memory and learning via CB1 activation in healthy brains in some mouse models.[8]
“According to anecdotal reports, an increased ratio of THC is required to increase the efficacy of some treatments. The range seems to vary significantly from 24:1 to 1:1 (CBD:THC) with fewer outlying cases reporting success from higher THC ratios.”
While this characteristic is not to be downplayed or overlooked, it should be pointed out that low doses of THC also activate preconditioning and postconditioning mechanisms that protect the brain from more severe insults.[8] This may be relevant because autistic brains are more vulnerable to environmental toxicity, oxidative stress, neuroinflammation, and neuronal insults.[4] That being said the possibility of adverse effects from cannabinoid therapies should be considered in pediatric patients. This is due to the concern of the unknown impact that cannabis treatments, particularly THC, has on a developing brain.
An argument could be made that botanical extracts with cannabidiol (CBD) present might offer safer options for patients, with greater clinical efficacy, when compared to THC alone.[7] This is partly why having access to CBD is important to ASD therapies, but it offers much more therapeutically than simply increasing the safety and efficacy of THC.[3]
While these articles cannot be taken as professional medical advice, the authors agree that based on the available data, generally speaking cannabis based therapies might only be warranted in the most severe cases of ASD, and only as a last-line therapy under the guidance of a qualified physician.
If a patient has a form of ASD that is truly severe, is unresponsive to available treatments, and the patient’s condition will deteriorate if no therapy is implemented, we believe that their family and physician should be legally permitted to make the decision as to whether botanical extracts from cannabis may be a viable option for treatment. Additionally, having access to both CBD and THC is optimal for the success of a cannabis therapy for ASD.
A Practical Approach to Cannabis Therapy
How can combinations of cannabinoids be put into practical use by individual families? For our purposes let’s review the anecdotal reports of cannabinoid based treatments currently being utilized in ASD as well as pediatric epilepsy. This might be a good comparison due to the range and complexity of both conditions and similarities in genetic dysfunctions. CBD-only extracts continue to prove effectiveness in treating many types of epilepsy, but not all.[6] According to anecdotal reports, an increased ratio of THC is required to increase the efficacy of some treatments. The range seems to vary significantly from 24:1 to 1:1 (CBD:THC) with fewer outlying cases reporting success from higher THC ratios.
Due to the range of ASD it seems possible that, similar to cannabinoid-based epilepsy treatments, varying ratios of cannabinoids (specifically CBD:THC) will prove to have a greater efficacy overall when compared to individual cannabinoid based treatments. The greater the ability to adjust the cannabinoid ratios the more optimal the conditions are to achieve therapeutic value. Though, generally speaking, they’re predominantly extracts that are high in CBD content.
“In ASD treatments, a first line of action to approaching a cannabis therapy might be to try a particularly high CBD ratio.”
In ASD treatments, a first line of action to approaching a cannabis therapy might be to try a particularly high CBD ratio. A high CBD containing botanical extract would be taken orally. The quantity of this botanical extract would slowly be increased incrementally based on weight until a desired effect, no effect, or an adverse effect is identified. If CBD alone is not sufficient to achieve a desired effect, a strain with higher content of THC is used, or an additional botanical extract that has a high THC content is added to a CBD extract in order to achieve the desired CBD:THC ratio. Again, this is incrementally increased based on weight until a desired effect, no effect, or an adverse effect is identified. More information on regiments can be found on Facebook in groups focusing on cannabis based pediatric therapies.
The ability to procure various ratios of cannabinoids in order to specifically tailor therapies may prove paramount to the effectiveness of treatments. Generally when parents find a strain or ratio that works well for them they try and stick with it. There are numerous cannabis varieties with varying ratios of cannabinoids in the majority of medical cannabis States. Seeking out plants that have been used in other ASD or epilepsy treatments might be a good first step.
Moving Forward
As future research is published we may see advances in the treatment of ASD by targeting the ECS. Until then we remain largely in the dark with possible glimmers of hope on the horizon. The mere possibility of combating ASD is enough for some families to explore cannabis as a treatment option, generally families unable to wait for possible future advances.
The question of when it becomes acceptable to provide a cannabis based treatment to a pediatric patient is complicated and loaded with moral and legal implications. The wide spectrum of ASD, the uncertainties in regards to targeting the endocannabinoid system for this treatment, and the possible adverse effects of THC therapy in pediatrics, all lend to the complexity of the issue.
In States with approved medical cannabis programs, it’s imperative that ASD be added to their lists of qualified medical conditions for approval of cannabis licenses. Parents and physicians should have the right and legal protection to explore cannabis as a treatment option, especially as a last-line therapy in ASD.
Citations & References
Földy, Csaba, Robert C. Malenka, and Thomas C. Südhof. "Autism-associated neuroligin-3 mutations commonly disrupt tonic endocannabinoid signaling." Neuron 78.3 (2013): 498-509.
Garcia, Arnau Busquets, et al. “New insights into the molecular pathophysiology of fragile X syndrome and therapeutic perspectives from the animal model”, International Journal of Biochemistry and Cell Biology, 53 (2014) 121-126.
Izzo, Angelo A., et al. "Non-psychotropic plant cannabinoids: new therapeutic opportunities from an ancient herb." Trends in pharmacological sciences 30.10 (2009): 515-527.
Kern, Janet K., and Anne M. Jones. "Evidence of toxicity, oxidative stress, and neuronal insult in autism." Journal of Toxicology and Environmental Health, Part B 9.6 (2006): 485-499
Malcher-Lopes, Renato. "Targeting alterations in the endocannabinoid system of rodents and non-human primates for the study of autism." Qatar Foundation Annual Research Conference. No. 2013. 2013.
Porter, Brenda E., and Catherine Jacobson. "Report of a parent survey of cannabidiol-enriched cannabis use in pediatric treatment-resistant epilepsy." Epilepsy & Behavior 29.3 (2013): 574-577.
Russo, Ethan, and Geoffrey W. Guy. "A tale of two cannabinoids: the therapeutic rationale for combining tetrahydrocannabinol and cannabidiol." Medical hypotheses2 (2006): 234-246.
Sarne, Yosef, et al. "The dual neuroprotective–neurotoxic profile of cannabinoid drugs." British journal of pharmacology 163.7 (2011): 1391-1401.
Siniscalco, Dario, et al. "Cannabinoid receptor type 2, but not type 1, is upregulated in peripheral blood mononuclear cells of children affected by autistic disorders." Journal of autism and developmental disorders 43.11 (2013): 26862695.
Zhang Longhua, Alger Bradley E., et al. “Enhanced Endocannabinoid Signaling Elevates Neuronal Excitability in Fragile X Syndrome” 2010
Additional Research Showing How Medical Cannabis Benefits ASD
- Consequences of cannabinoid and monoaminergic system disruption in a mouse model of autism spectrum disorders [http://www.ncbi.nlm.nih.gov/pubmed/21886592]
Conclusion For Adding The Medical Condition: Autism Spectrum Disorders
The approval of this petition would promote health and wellness, improve health outcomes for people and families with ASD, and assures a safety net of services from the Medical Cannabis Program Office for all people in New Mexico by the Department of Health. Approval of this Petition furthers the intent of the law and continues to uphold the spirit of the Lynn and Erin Compassionate Use Act, 2007. Fulfilling both;“ Section 2. PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments” And Section 6. ADVISORY BOARD CREATED--DUTIES: The advisory board shall: A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis.” New Mexico’s medical cannabis history started in 1978, 40 years ago this year...after public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis...the first law.
Petition Can Be Viewed Online At: LECUA NM MCP MCAB Petitions (http://lecuanmmcpmcabpetitions.blogspot.com/)

No comments:
Post a Comment