
Jason Barker - Medical Cannabis Patient & Organizer with LECUA Patient’s Coalition Of New Mexico
dukecitywellness.blogspot.com
Tuesday, February 28th 2017
New Mexico State Department of Health
Medical Cannabis Advisory Board
Medical Cannabis Program
PO Box 26110
Santa Fe, NM, 87502-6110
Medical Cannabis Program
PO Box 26110
Santa Fe, NM, 87502-6110
Medical Cannabis Advisory Board Petition for the Medical Treatment; Adequate Supply:
Remove CBD from Plant Count
Table of Contents
Pg. 1 Cover Page
Pg. 2 - 4 Petition Introduction
Pg. 4 - 9 Petition Purpose and Background
Pg. 9 - 11 Relief Requested In Petition
Pg. 11 References
Pg. 12-14 Appendix A
Pg. 14-17 Appendix B
Printing Provided By:

Petition Introduction: Requesting for the Medical Treatment; Adequate Supply: Remove CBD from Plant Count
New Mexico’s medical cannabis history started in 1978, after public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis. The New Mexico’s medical cannabis program (MCP) is the only program in the U.S. that places sole responsibility for regulation on the state’s Department of Health. Doctors must comply with state requirements for patients to be considered for applying to the medical cannabis program.
The Santa Fe New Mexican reported on February 13th (2017) that the New Mexico Medical Cannabis program has grown dramatically from 9,000 patients in 2013 to more than 33,000 today. The Department of Health estimates approximately 500 to 800 new patients join the program weekly. The tremendous growth of the Medical Cannabis Program with new program participants, an increase of 75% during 2016, so that currently means we have almost 45,000 patients benefiting from medical cannabis. The medical cannabis program office is currently processing applications in a 12-14 day range and recommends submitting renewal and new patient applications a minimum of 60 days prior to expiration to allow ample time for processing. Due to the incredible growth in the medical cannabis program participants, there needs to be a clear increase to the plant count allowed for by the licensed producers from the Department of Health. In order for the Department of Health Medical Cannabis Program to allow for the beneficial treatment with medical cannabis, the Department must properly have “adequate supply”.
There are 35 licensed producers growing medical cannabis, operating 41 dispensaries around the state, and 23 of these dispensaries are located in the Albuquerque area. Current state law does not limit the number of plants that can be grown by the state’s licensed producers. Each one of the licensed producers is can choose to grow up to 450 medical cannabis plants, the maximum allowed under the Department of Health program rules and regulations. The department may issue two classes of producer licenses; to a qualified patient who holds a valid personal production license and to a non-profit producer who operates a facility.
The 2016/17 licensure list for the medical cannabis program shows a total of 13,800 medical cannabis plants licensed by the 35 producers for the All patients in the program.
In the Lynn and Erin Compassionate Use Act, (2007) the law states; The Secretary of Health shall establish an advisory board consisting of eight practitioners representing the fields of neurology, pain management, medical oncology, psychiatry, infectious disease, family medicine and gynecology. The practitioners shall be nationally board-certified in their area of specialty and knowledgeable about the medical use of cannabis. The members shall be chosen for appointment by the Secretary from a list proposed by the New Mexico Medical Society. A quorum of the advisory board shall consist of three members.
The advisory board shall:
A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis;
B. accept and review petitions to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
C. convene at least twice per year to conduct public hearings and to evaluate petitions, which shall be maintained as confidential personal health information, to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
D. issue recommendations concerning rules to be promulgated for the issuance of the registry identification cards; and
E. recommend quantities of cannabis that are necessary to constitute an adequate supply for qualified patients and primary caregivers.
First, do no harm. As an important step in becoming a doctor, medical students must take the Hippocratic Oath. And one of the promises within that oath is “first, do no harm”.
A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis;
B. accept and review petitions to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
C. convene at least twice per year to conduct public hearings and to evaluate petitions, which shall be maintained as confidential personal health information, to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
D. issue recommendations concerning rules to be promulgated for the issuance of the registry identification cards; and
E. recommend quantities of cannabis that are necessary to constitute an adequate supply for qualified patients and primary caregivers.
First, do no harm. As an important step in becoming a doctor, medical students must take the Hippocratic Oath. And one of the promises within that oath is “first, do no harm”.
Dr. William Johnson, former chair of the New Mexico Medical Cannabis Advisory Board in 2014 told KUNM public radio that many of the changes proposed by the Department of Health would hurt patient access to medical cannabis. After the Rules and Regulations changes from the medical cannabis meetings in 2014 went into effect in February of 2015, the results for patients and caregivers in the program has been clearly harmful to patient well being and overall program health. And it is the patient’s, producers, and medical cannabis community members that are now paying the price in regards to health and financial costs.
We have a sound law in the Lynn and Erin Compassionate Use Act, yet we are unable to provide “adequate supply” and it can not be properly defined by the Department by using unknown variables it has not collected then this leads to further examination of how these definitions pertaining to adequate supply were determined in the past years.
We have a sound law in the Lynn and Erin Compassionate Use Act, yet we are unable to provide “adequate supply” and it can not be properly defined by the Department by using unknown variables it has not collected then this leads to further examination of how these definitions pertaining to adequate supply were determined in the past years.
In order for the Department of Health Medical Cannabis Program to allow for the medical treatment of cannabis, the Department must properly have “adequate supply”. For the Department to have “adequate supply” they would need to know the different amounts of plant material that goes into all the different types of medicine being produced in the MCP. Dried cannabis flower (bud), pre-rolls, edibles, tinctures, topicals/salves, and concentrated forms of cannabis- all require different amounts of cannabis plant material to produce. This is empirical data that has not been collected, studied or researched within the state’s medical cannabis program by the Department of Health.
The current law for the Medical Cannabis Program, passed in 2007, states the following, (Page 1/Section 2) “PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.”
How is the purpose of the law able to be fulfilled without knowing Adequate Supply and by preventing patients from properly treating themselves due to adequate supply limits?
Section 2. PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
“ARTICLE 2B. LYNN AND ERIN COMPASSIONATE USE ACT
N.M. Stat. Ann. § 26-2B-2 (2009)
§ 26-2B-2. Purpose of act
The purpose of the Lynn and Erin Compassionate Use Act [26-2B-1 NMSA 1978] is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
HISTORY: Laws 2007, ch. 210, § 2.
EFFECTIVE DATES. --Laws 2007, ch. 210, § 12 makes the act effective July 1, 2007.”
Mosby’s Medical Dictionary states that “medical treatment” means; the management and care of a patient to combat disease or disorder. Medical treatment includes: Using prescription medications, or use of a non-prescription drug at prescription strength; and or treatment of disease by hygienic and pharmacologic remedies, as distinguished from invasive surgical procedures. Treatment may be pharmacologic, using drugs; surgical, involving operative procedures; or supportive, building the patient's strength. It may be specific for the disorder, or symptomatic to relieve symptoms without effecting a cure.(Mosby's Medical Dictionary, 9th edition.)
What is a chronic medical condition?
A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear. Harvard Medical Dictionary defines chronic as: Any condition that lasts a long time or recurs over time; chronic pain as: Pain that persists after an injury has healed or a disease is over; and chronic pain syndrome as : Long-term, severe pain that doesn't spring from an injury or illness, that interferes with daily life, and is often accompanied by other problems, such as depression, irritability, and anxiety.
A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear. Harvard Medical Dictionary defines chronic as: Any condition that lasts a long time or recurs over time; chronic pain as: Pain that persists after an injury has healed or a disease is over; and chronic pain syndrome as : Long-term, severe pain that doesn't spring from an injury or illness, that interferes with daily life, and is often accompanied by other problems, such as depression, irritability, and anxiety.
What is the meaning of debilitating?
Something that's debilitating seriously affects someone or something's strength or ability to carry on with regular activities, like a debilitating illness. Debilitating comes from the Latin word debilis, meaning "weak." That's why you'll often see the adjective used to describe illness, despite the negative reference.
Something that's debilitating seriously affects someone or something's strength or ability to carry on with regular activities, like a debilitating illness. Debilitating comes from the Latin word debilis, meaning "weak." That's why you'll often see the adjective used to describe illness, despite the negative reference.
Petition Purpose And Background
The purpose of this petition is Requesting for the Medical Treatment; Adequate Supply: Remove CBD from Plant Count.
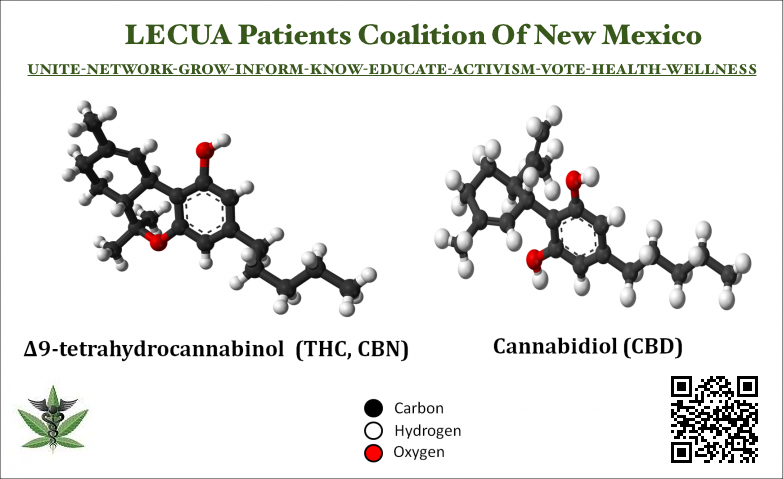
Cannabidiol (CBD) is one of at least 113 active cannabinoids identified in cannabis. It is a major phytocannabinoid, accounting for up to 40% of the plant's extract.
The MCP should have a Plant Count that is based on ratio of patients to serve AND inclusion of empirical data for all varying amounts medical cannabis plant material needed to manufacture different forms of medical cannabis medicine.
Medical Cannabis / HEMP CBD strains at ratio of; 1.5 THC (or lower) : 1 CBD (or higher) should be removed from the Plant Count for Patient/Caregiver PPL and LNPP allowable plant count.
This petition Requesting for the Medical Treatment; Adequate Supply: Remove CBD from Plant Count, is being provided to bring the state Department of Health Medical Cannabis Program in compliance with the Lynn and Erin Compassionate Use Act.
Removing CBD strains from cannabis plants counts in New Mexico and other state programs for patients, caregivers and medical cannabis producers allowable plant count just makes sense. A patent was already awarded to part of the federal government, the U.S. Health and Human Services in 2003 (US6630507) that also covers the use of CBD as a treatment for various neurodegenerative and inflammatory disorders. Since cannabis contains medicinal compounds recognized and endorsed by an agency of the U.S. government- Why is it that cannabis remains on the Federal Schedule One list of drugs?
The fact that CBD-rich cannabis is non-psychoactive or less psychoactive than THC-dominant strains makes it a great option for patients looking for relief without disconcerting feelings of lethargy or dysphoria.
Removing CBD plant strains from the state’s program plant counts would allow for the proposed 5 ounces monthly in adequate supply for patients. This would also allow for patients with a personal production license to empower themselves and their own grows with more CBD cannabis plants. For the LNPP growing medical cannabis, this would allow for 450 THC medical cannabis plants while still being able to provide enough CBD medical cannabis plants - thus allowing for the growing of a larger variety of medical cannabis strains and enable the CBD needs for patients to be easily achieved by producers. Removing the CBD, at the suggested ratio above, would allow LNPP in the program to producer a larger variety of medicine for all the qualifying health conditions.
Examples of Medical Cannabis THC Strains For Pain Relief
Generally, cannabis strains with high percentage of cannabis compounds, cannabidiol (CBD) and tetrahydrocannabinol (THC), are most effective at pain relief. For this reason, Blueberry Kush, a hybrid strain that features a blueberry aroma and dark green buds, has been widely used as part of a pain management regimen. Another strain that's been getting attention when it comes to generalized pain is the Auto White Widow. Both of these strains work well for general pain.
To treat migraines, Grand Daddy Purple is an indica strain that delivers cerebral euphoria to relieve headaches. Similarly, many migraine sufferers swear by the pain-relieving properties of Blue Dream. This hybrid strain can ease the user into cerebral invigoration and body relaxation.
For those suffering from arthritis, AK-47 is a popular strain with a high THC content. This sativa-dominant strain provides alertness along with pain relief. Master Kush has been doing wonders for patients suffering from arthritic pain as well. This strain provides a visual high before gradually providing full-body relaxation.
Acapulco Gold is widely used by women suffering from menstrual cramps. This plant has buds that resemble gold and a 23 percent THC content. Alaskan Ice is another option to consider, as this potent sativa strain provides a euphoric high.
Critical Mass is a combination of Skunk # 1 and Afghani and has a THC level of 19 to 22 percent, making it a good choice for treating fibromyalgia pain. Ace of Spades is another strain to consider for a wide range of medical benefits in addition to alleviating fibromyalgia pain.
Patients suffering from spinal injury will like the euphoria-inducing effect of Purple Haze. This purplish plant has green and orange undertones with an earthy smell. Alternately, Khalifa Kush is also a good option for those who wants to be up and running all throughout the day, as it provides an energy boost. This medical cannabis also leaves the patient with distinct cerebral buzz to help alleviate the pain.
Mendo Purps is an indica-dominant cannabis strain used to treat multiple sclerosis. It can also relieve muscle spasms and fatigue. Novice cannabis user who want the therapeutic effects of medical cannabis can also try Bhang Skywalker OG, a strain with coconut oil that's infused with 25 to 35 percent THC, making it a strong sedative and a popular pain reliever. [https://www.hellomd.com/health-wellness/cannabis-strains-for-different-kinds-of-pain]
Medical Cannabis CBD & Hemp CBD strains at ratio of; 1.5 thc (or lower) : 1 cbd (or higher) should not be counted against total allowed medical cannabis plants for the Patient PPL and the LNPP allowable plant count. And the establishment of an monthly allotment for Clones and Cuttings provided to qualified patient / caregiver with a PPL by a LNPP’s should not counted against LNPP allowable plant count.
In order for the Department of Health Medical Cannabis Program allow for the medical treatment of cannabis, the Department must properly have “adequate supply”. For the Department to have “adequate supply” they would need to know the different amounts of plant material that goes into all the different types of medicine being produced. Dried cannabis flower (bud), pre-rolls, edibles, tinctures, topicals/salves, and concentrated forms of cannabis all require different amounts of cannabis plant material to produce.
This is empirical data that has not been collected within the state’s medical cannabis program by the Department of Health. Therefore “adequate supply” can not be properly defined by the department by using unknown variables it has not collected. This further prevents the Department of Health from being able to set a proper plant count for each producer in the program for the means of achieving adequate supply within the medical cannabis program as required by law.
Medical cannabis patients registered in the New Mexico MCP use the different kinds of cannabis oil with all types of conditions including, but not limited to, Amyotrophic Lateral Sclerosis (ALS), Cancer, Crohn’s Disease, Epilepsy, Glaucoma, Hepatitis C, HIV/AIDS, Huntington’s Disease, Hospice Care, Inclusion Body Myositis, Inflammatory, Autoimmune-mediated Arthritis, Multiple Sclerosis, Damage to the nervous tissue of the spinal cord, Painful peripheral neuropathy, Parkinson’s disease, Post-Traumatic Stress Disorder (PTSD), Severe Chronic Pain, Severe Anorexia/Cachexia, Spasmodic Torticollis (Cervical Dystonia), Ulcerative Colitis, arthritis, diabetes, depression, osteoporosis, psoriasis, insomnia, asthma, burns, migraines, regulation of body weight, chronic pain, and mutated cells (polyps, warts, tumors).
Cannabinoids and Therapeutic Effects: CBD
Cannabidiol, CBD, is a cannabis compound that has significant medical benefits, but does not make people have the euphoric feeling of being “stoned” and can actually counteract that psychoactivity aspect of THC. The fact that CBD-rich cannabis is non-psychoactive or less psychoactive than THC-dominant strains makes it a great option for patients looking for relief without disconcerting feelings of lethargy or dysphoria.
CBD is a key ingredient in cannabis and is one of more than 80 active cannabinoid compounds found in the cannabis plant that belong to a class of molecules called cannabinoids. Of these compounds, CBD and THC are usually present in the highest concentrations, and are therefore the most recognized and studied. CBD and THC levels tend to vary among different plants. Cannabis grown for recreational purposes often contains more THC than CBD.
However, by using selective breeding techniques, cannabis breeders have managed to create varieties with high levels of CBD and next to zero levels of THC. These strains are rare but have become more popular in recent years.
The beneficial health effects of CBD for the human body are coming more and more prevalent into social awareness, here are five facts that you should know about this unique compound:
1. CBD is Non-Psychoactive:
Unlike THC, CBD does not cause a “high”. While this makes CBD a poor choice for recreational users, it gives the chemical a significant advantage as a medicine, since health professionals prefer treatments with minimal side effects. CBD is non-psychoactive because it does not act on the same pathways as THC. These pathways, called CB1 receptors, are highly concentrated in the brain and are responsible for the mind-altering effects of THC. A 2011 review published in Current Drug Safety concludes that CBD “does not interfere with several psychomotor and psychological functions.” The authors add that several studies suggest that CBD is “well tolerated and safe” even at high doses.
2. CBD can Treat Addiction:
Drug addiction is a disorder characterized by the compulsive and uncontrollable desire to use drugs. A 2013 animal study published in Addictive Biology found CBD inhibits the rewarding effect of morphine. CBD was able to block morphine’s addictive effect on the rats by reducing the pleasure the drug offered. CBD is an exogenous cannabinoid that acts on several neurotransmission
systems involved in addiction. Scientific studies have shown the beneficial effects of CBD on opioid and other psychostimulant addictions.
systems involved in addiction. Scientific studies have shown the beneficial effects of CBD on opioid and other psychostimulant addictions.
3. CBD helps Regulate Blood Sugar Levels in the Body
Studies as recent as 2013 have found that one of the ways that cannabis helps people regulate their weight is through regulating blood sugar levels. Studies found that cannabis users were less likely to develop diabetes in their life. As to whether or not CBD is useful for diabetes patients is still somewhat controversial but more studies are being done to show these benefits. But CBD regulates blood sugar levels and decreases the likelihood of developing diabetes.
4. CBD Treats and Reduces Seizures In Children
CBD has anti-seizure activity, reducing the severity of seizures in animal studies. Several case studies and reports suggest CBD is effective in treating children with drug-resistant epilepsy. Charlotte's Web is one strain of cannabis create just for this purpose.
5. CBD Inhibits Cancer Cell Growth
The cannabinoids in marijuana excite certain receptors that allow the body to produce pharmacological effects in the immune system and the central nervous system. Cannabinoids have been found to act in this way to inhibit cancer cell growth. In fact, they are being used to decrease the size of tumors also, and for cancer-related side effects. CBD has been shown to reduce pain and nausea, and increase appetite during patients' cancer treatments. There are also reports that show CBD's anti-tumor effects. There has been a reduced cell viability, increased cancer cell death, decreased tumor growth, and inhibition of metastasis. Researchers attribute these effects to to the antioxidant and anti-inflammatory properties of CBD. Combined with the THC cancer killing effect, this is really a big deal underscored by the US Government and Big Pharma!
CBD has demonstrated neuroprotective and neurogenic effects, and its anti-cancer properties are currently being investigated at several academic research centers in the United States and elsewhere. Although CBD and THC act on different pathways of the body, they seem to have many of the same medical benefits. According to a 2013 review published in the British Journal of Clinical Pharmacology, studies have found CBD to possess the following medical properties:
Medical Properties of CBD
|
Effects
|
Antiemetic
|
Reduces nausea and vomiting
|
Anticonvulsant
|
Suppresses seizure activity
|
Antipsychotic
|
Combats psychosis disorders
|
Anti-inflammatory
|
Combats inflammatory disorders
|
Anti-oxidant
|
Combats neurodegenerative disorders
|
Anti-tumoral/Anti-cancer
|
Combats tumor and cancer cells
|
Anxiolytic/Anti-depressant
|
Combats anxiety and depression disorders
|
While some doctors can’t seem to look past certain effects of THC due to a lack of general understanding of cannabis, CBD doesn’t appear to present that much of problem. More and more evidence of CBD’s medical benefits continues to grow with CBD’s potential as a treatment for a wide range of conditions, including anxiety, arthritis, diabetes, addiction, alcoholism, MS, chronic pain, schizophrenia, PTSD, depression, antibiotic-resistant infections, epilepsy, and many other neurological disorders.
A patent awarded to the U.S. Health and Human Services in 2003 (US6630507) also covers the use of CBD as a treatment for various neurodegenerative and inflammatory disor
Rules, Regulations, & Policy Solution - Requesting for the Medical Treatment; Adequate Supply: Remove CBD from Plant Count
For ensuring safe access to all areas of the the state of New Mexico and proper administering of the Lynn and Erin Compassionate Use Act, by the New Mexico State Department of Health, this can be achieved by making revisions to licensing requirements for medical cannabis licensed producers with a plant count for patients and producers properly structured and increased: Medical cannabis CBD strains at ratio of; 1.5 thc(or lower) : 1 cbd (or higher) being removed from patient or producer allowable plant count;
First, not all medical cannabis plants are the same. The cannabis plant contains dozens of cannabinoids. The most well known cannabinoid for a long time has been tetrahydrocannabinol (THC), but as more scientific research is conducted involving cannabis and its ability to be used as a medicine, more and more people are learning about other cannabinoids, especially cannabidiol (CBD). Some plants have THC and others produce CBD, THC has psychoactive properties that affect your brain and give you a ‘runner’s high’ while CBD does not.
Making revisions to licensing requirements for medical cannabis licensed producers with a plant count for patients and producers properly structured and increased: Medical cannabis CBD strains at ratio of; 1.5 thc(or lower) : 1 cbd (or higher) being removed from patient or producer allowable plant count.
Medical cannabis clones and cuttings provided to qualified patient with a personal production license by a licensed producer should not count against the maximum allowable plant count. A plant count that is based on ratio of patients to serve with inclusion of empirical data for varying amounts cannabis plant material needed to manufacture different forms of medical cannabis medicine.
A plant count to provide a ratio of 3 THC medical cannabis plants per enrolled patient in conjunction with medical cannabis CBD strains having been removed from the plant count. And based on yearly program totals. Thus, if there were 40,000 patients plus the 3 cannabis plants would equal 120,000 THC medical cannabis plants for 35 licensed producers equals 3,429 allowable medical cannabis plants (Minimum standard set by MCAB & Plant Count adjusted yearly for program growth). Plant count increase structured to be 1715 plant increase by July 1st 2017 then another 1714 by July 1st 2018. Structuring this in phases will reduce the risk of crop problems and maintain high standards of quality for the medical cannabis plants.
Licensing fee structure changed and lowered to be as follows; the department shall assess a nonrefundable fee not greater than five hundred dollars ($500) for processing an application for a new or renewal license. For a new or renewal processor license, medical wholesale license or medical retail license, the department shall charge an annual license fee of not more than two thousand dollars ($2,000). For a new or renewal production license, the department shall charge an annual license fee of: Fifteen thousand dollars ($15,000), if the producer will possess up to one hundred fifty cannabis plants; and an additional five thousand dollars ($5,000) for each additional fifty cannabis plants the producer will possess. And this also will prevent a small number of the licensed producers from cornering the market of medical cannabis.
The per plant fee would be $100 for medical cannabis plants containing a THC content above the provided CBD ratio. Licensure limit established allowing one licensed producer to have one grow location per three dispensary store fronts whereas current rules and regulation do not limit this. All current producers would be granted additional license(s) per application review and program performance standards met. A time period for new producers to open needs to be established; 90-120 window of days then letter sent providing a warning and 45 days time, then final letter sent providing 30 days before forfeiture of license.
A plant count structure like this petition that is Requesting for the Medical Treatment; Adequate Supply: Remove CBD from Plant Count; would bring the state of New Mexico and the Department of Health in compliance with the intent of the law and uphold the spirit of the Lynn and Erin Compassionate Use Act, 2007. New Mexico’s medical cannabis history started in 1978. After public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis...the first law. The Department of Health should additional employ three staff members to provide medical cannabis health education statewide. The Department of Health should also establish a training and certification program for all dispensary employees.
As pointed out, in order for the Department of Health Medical Cannabis Program to allow for the medical treatment of cannabis, the Department must properly have “adequate supply” and have it properly defined. And for the Department to have “adequate supply” they would need to know the different amounts of plant material that goes into all the different types of medicine being produced. Dried cannabis flower (bud), pre-rolls, edibles, tinctures, topicals/salves, and concentrated forms of cannabis all require different amounts of cannabis plant material to produce. Adequate Supply can not have a set definition in the rules and regulations and needs to be reviewed to coincide with MCP growth and patient/caregiver needs. Adequate Supply should be reviewed quarterly (4 times per year) with a current census completed of qualified patients, caregivers and licensed non-profit producers.
(Ad·e·quate: (ˈadəkwət/) adjective; satisfactory or acceptable in quality or quantity.
Sup·ply (səˈplī/) verb; 1. make (something needed or wanted) available to someone; provide.
"the farm supplies apples to cider makers" or a noun; 1. a stock of a resource from which a person or place can be provided with the necessary amount of that resource.) [https://www.merriam-webster.com/]
"the farm supplies apples to cider makers" or a noun; 1. a stock of a resource from which a person or place can be provided with the necessary amount of that resource.) [https://www.merriam-webster.com/]
This is empirical data that has not been collected within the state’s medical cannabis program by the Department of Health. Therefore “adequate supply” can not be properly defined by the department by using unknown variables it has not collected. This further prevents the Department of Health from being able to set a proper plant count for each kind of licensed producer in the program for the means of achieving adequate supply within the medical cannabis program as required by law.
This is empirical data has been studied and researched by the state of Colorado by the Colorado Department of Revenue: “An assessment of physical and pharmacokinetic relationships in marijuana production and consumption in Colorado”.
How is the purpose of the law able to be fulfilled without knowing Adequate Supply and by preventing patients from properly treating themselves due to adequate supply limits?
Section 2. PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
“ARTICLE 2B. LYNN AND ERIN COMPASSIONATE USE ACT
N.M. Stat. Ann. § 26-2B-2 (2009)
§ 26-2B-2. Purpose of act
The purpose of the Lynn and Erin Compassionate Use Act [26-2B-1 NMSA 1978] is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
HISTORY: Laws 2007, ch. 210, § 2.
EFFECTIVE DATES. --Laws 2007, ch. 210, § 12 makes the act effective July 1, 2007.”
References
The solution provided above was derived from the following sources:
Americans For Safe Access [http://www.safeaccessnow.org/policy_shop], Colorado Medical Marijuana Program [https://www.colorado.gov/pacific/cdphe/medicalmarijuana], Colorado Department of Revenue- An assessment of physical and pharmacokinetic relationships in marijuana production and consumption in Colorado [https://www.colorado.gov/pacific/sites/default/files/MED%20Equivalency_Final%2008102015.pdf], Cannabis Yields and Dosing by Chris Conrad (court qualified cannabis expert) [http://chrisconrad.com/], and the Hawaii Medical Cannabis Program-Medical Marijuana Dispensary Task Force Study 2015 [http://files.hawaii.gov/auditor/Reports/2014/14-12.pdf].
Appendix A:
ASA Releases Federal Medical Cannabis Policy Roadmap
[http://www.safeaccessnow.org/briefingbook115]
An Americans for Safe Access (ASA) national report was released on December 8th, 2016 and calls for an end to contradictions between federal and state guidelines with regard to medical cannabis policies. The Americans for Safe Access briefing book, “Medical Cannabis in America”, showing that not only do opiate related deaths drop an average of 24.8% in states with medical cannabis laws, the report also notes that the Department of Justice has spent an estimated $592 million to date in arrests, investigations, enforcement raids, pretrial services, incarceration, and probation.
The report includes actions for the POTUS during the lame duck as well as the incoming Congress and POTUS. These actions would protect the more than 2 million medical cannabis patients in the U.S. by allowing local manufacturers, growers, and distributors to operate in accordance with their own state’s laws regarding medical cannabis without fear of federal interference.
“Medical cannabis is reshaping the way we view modern medicine,” Steph Sherer, ASA’s executive director said in a written statement. “But in order to continue providing millions of patients with the medicine they need, Congress and the Obama Administration need to take action.” Most importantly there are things that President Obama can do before he leaves office to ensure a smoother transition for medical cannabis policy under the new administration. This is perhaps one of the only political issues that has bipartisan support.
‘Medical Cannabis in America: The Medical Cannabis Briefing Book’ is a guidebook for Congress and the Administration that includes information on modern scientific evidence about medical cannabis, what the federal and state conflict means for patients who rely on this medicine, and what Congress can do to end this conflict.
‘Medical Cannabis in America: The Medical Cannabis Briefing Book’ is a guidebook for Congress and the Administration that includes information on modern scientific evidence about medical cannabis, what the federal and state conflict means for patients who rely on this medicine, and what Congress can do to end this conflict.
The report outlines how federal agencies can help states to increase the quality and safety of medical cannabis programs, details a role for federal oversight after the passage of comprehensive legislation and outlines the following steps:
*Instruct Drug Enforcement Administration (DEA) to update their website and publications to reflect their most current science.
*Order Health and Human Services (HHS) and DEA to take the recommendation from Food and Drug *Administration (FDA) Acting Commissioner Stephen Ostroff to examine and possibly overhaul the regulations that are preventing medical research and rescheduling of cannabis.
*Engage with U.N. Secretary General on the scheduling of cannabis in the UN Single Convention of Drugs, which is based on a report from 1935.
*Release the remaining medical cannabis POWs and drop the handful of remaining prosecutions.
*Instruct Drug Enforcement Administration (DEA) to update their website and publications to reflect their most current science.
*Order Health and Human Services (HHS) and DEA to take the recommendation from Food and Drug *Administration (FDA) Acting Commissioner Stephen Ostroff to examine and possibly overhaul the regulations that are preventing medical research and rescheduling of cannabis.
*Engage with U.N. Secretary General on the scheduling of cannabis in the UN Single Convention of Drugs, which is based on a report from 1935.
*Release the remaining medical cannabis POWs and drop the handful of remaining prosecutions.
“Medical Cannabis in America: The Medical Cannabis Briefing Book” also dispels a number of popular myths about cannabis - amongst them that cannabis is a “gateway” drug, and documents how over 2 million Americans rely on state-run, physician supervised cannabis programs to alleviate symptoms of illnesses like cancer, crohn’s disease, multiple sclerosis, parkinson’s, seizure disorders, post traumatic stress, and chronic pain.
The report shows that:
*Opiate related deaths dropped an average of 24.8% in states with medical cannabis laws.
*89% of Americans support medical cannabis.
*The Department of Justice (DOJ) has spent an estimated $592 million to date in arrests, investigations, enforcement raids, pretrial services, incarceration, and probation.
*The total amount spent on federal interference under the Bush Administration two terms was estimated to be in excess of $232 million — The Obama Administration two terms has spent $350 million.
*In 2012 the DEA used 5% of their budget on medical cannabis cases.
*There are 44 states with medical cannabis laws.
*Opiate related deaths dropped an average of 24.8% in states with medical cannabis laws.
*89% of Americans support medical cannabis.
*The Department of Justice (DOJ) has spent an estimated $592 million to date in arrests, investigations, enforcement raids, pretrial services, incarceration, and probation.
*The total amount spent on federal interference under the Bush Administration two terms was estimated to be in excess of $232 million — The Obama Administration two terms has spent $350 million.
*In 2012 the DEA used 5% of their budget on medical cannabis cases.
*There are 44 states with medical cannabis laws.
“The next Congress must pass the CARERS Act or its successor bill to protect millions of patients from federal interference in states with medical cannabis programs,” said Mike Liszewski, Director of Government Affairs at Americans for Safe Access. “CARERS has the potential to greatly improve public health by harmonizing state and federal medical cannabis laws, but we need our elected officials to act swiftly. Millions of people depend on this botanical medicine and simply cannot afford to wait.”
There are 128,000 opiate related deaths annually as opposed to 0 deaths caused by cannabis. The ASA recommendations include reflecting the most current science across DEA platforms and overhauling regulations that prevent medical marijuana research. In order to protect medical cannabis patients in the U.S. we must help manufacturers, growers, and distributors to operate without fear of federal interference.
It’s really important for all people within the cannabis community to know, they are the power; the government, legislators & policy makers are lead to us and “We the people” have the power to change the laws and government - people in it, policy being written, and overturning rules & regulations that disrupt safe access to cannabis. Not one state’s medical cannabis program or legalization law is perfect, they are working pieces of democracy. Good policy is created when those who are most affected are at the table, please send copies of the “The Medical Cannabis Briefing Book” and US Patent #6,630,507 “Cannabinoids as Antioxidants and Neuroprotectants” to your elected officials, and local media today!
About Americans for Safe Access.
The mission of Americans for Safe Access (ASA) is to ensure safe and legal access to cannabis for therapeutic use and research. ASA was founded in 2002, by medical cannabis patient Steph Sherer, as a vehicle for patients to advocate for the acceptance of cannabis as medicine. With over 100,000 active members in all 50 states, ASA is the largest national member-based organization of patients, medical professionals, scientists and concerned citizens promoting safe and legal access to cannabis for therapeutic use and research. ASA works to overcome political, social and legal barriers by creating policies that improve access to medical cannabis for patients and researchers through legislation, education, litigation, research, grassroots empowerment, advocacy and services for patients, government's, medical professionals, and medical cannabis providers.
The mission of Americans for Safe Access (ASA) is to ensure safe and legal access to cannabis for therapeutic use and research. ASA was founded in 2002, by medical cannabis patient Steph Sherer, as a vehicle for patients to advocate for the acceptance of cannabis as medicine. With over 100,000 active members in all 50 states, ASA is the largest national member-based organization of patients, medical professionals, scientists and concerned citizens promoting safe and legal access to cannabis for therapeutic use and research. ASA works to overcome political, social and legal barriers by creating policies that improve access to medical cannabis for patients and researchers through legislation, education, litigation, research, grassroots empowerment, advocacy and services for patients, government's, medical professionals, and medical cannabis providers.
Plant Count For Producers Based On Patient Population Growth For Adequate Supply Proposed: Legislators and the Department could easily solve this by looking to Americans For Safe Access for this policy.
Appendix B: Relief Requested (Outline)
For ensuring safe access to all areas of the the state of New Mexico and proper administering of the Lynn and Erin Compassionate Use Act, by the New Mexico State Department of Health can be achieved with “adequate supply” as follows:
- Adequate supply of medical cannabis properly defined, structured, and increased.
- Maximum quantity of usable cannabis increased to 425.243 grams per 3 months ( 2.5 ounces every two weeks ).
- Inclusion of empirical data for for determining adequate supply for varying amounts cannabis plant material needed to manufacture different forms of medical cannabis medicine for proper dosage.
- Revisions to licensing requirements for MCP LNPP’s
- Plant count for patients & producers properly structured and increased.
- Cannabis CBD strains at ratio of; 1.5 thc (or lower) : 1 cbd (or higher) not counted against patient/caregiver or LNPP allowable plant count.
- Clones and Cuttings provided to qualified patient / caregiver with a PPL by a LNPP’s not counted against LNPP allowable plant count.
- Plant Count that is based on ratio of patients to serve AND inclusion of empirical data for varying amounts cannabis plant material needed to manufacture different forms of medical cannabis medicine.
- Patient / Caregiver PPL plant count increased to allow for 6 immature seedlings /clones / cuttings, 6 plants in vegetative stage, and 6 plants in flowering stage for total of 18 cannabis plants.
- The addition of Cooperative/Collective PPL’s
- Whereas Rules and Regulations for Personal Production License should additionally include:
The Department shall issue a individual cultivation registration to a qualifying patient or their personal caregiver. No more than 4 qualified patients may collectively cultivate 60 medical cannabis plants, and each participating patient must obtain a collective cultivation registration. The Department may deny a registration based on the provision of false information by the applicant. Such registration shall allow the qualifying patient or their personal caregiver to cultivate an area of limited square footage of plant canopy, sufficient to maintain a 90-day supply of cannabis, and shall require cultivation and storage only in a restricted access area.
A qualifying patient or personal caregiver shall not be considered to be in possession of more than a 90-day supply at the location of a restricted access area used collectively by more than one patient, so long as the total amount of cannabis within the restricted access area is not more than a 90-supply for all the participating qualifying patients. A copy of each qualifying patient’s written recommendation shall be retained at the shared cultivation facility - Qualified patients shall provide the following in order to be considered for a personal production license to produce medical cannabis:
(1) a description of the single indoor or outdoor location that shall be used in the production of cannabis;
(2) a written plan that ensures that the cannabis production shall not be visible from the street or other public areas; - (3) a written acknowledgement that the applicant will ensure that all cannabis, cannabis-derived products and paraphernalia is accessible only by the applicant, collective members and/or their primary caregiver (if any), and kept secure and out of reach of children;
- (4) a description of any device or series of devices that shall be used to provide security and proof of the secure grounds; and
(5) a written acknowledgement of the limitations of the right to use and possess cannabis for medical purposes in New Mexico. - ”Cultivation facility” means a business that:
1. Is registered with the Department of Agriculture; and (we should be having Dept. of Ag involved)
2. Acquires, possesses, cultivates, harvests, dries, cures, trims, and packages cannabis and other related supplies for the purpose of delivery, transfer, transport, supply, or sales to:
(a) dispensing facilities;
(b) processing facilities;
(c) manufacturing facilities;
(d) other cultivation facilities;
(e) research facilities.
(f) independent testing laboratories.
- LNPP Plant Count maximum ratio of 3 cannabis plants per enrolled patient. Based on yearly program totals. Thus; 30,000 patients x 3 cannabis plants = 90,000 cannabis plants / 35 LNPP = 2,571.43 max allowable cannabis plants per LNPP. ( Minimum standard set by MCAB / Plant Count adjusted yearly for program growth )
- Plant count increase structured : 1000 plants by July 1st 2017 then 2000 by July 1st 2018 and then 571 by July 2019
- Licensing fee structure changed and lowered.
- The department shall assess a nonrefundable fee not greater than five hundred dollars ($500) for processing an application for a new or renewal license.
- For a new or renewal processor license, medical wholesale license or medical retail license, the department shall charge an annual license fee of not more than two thousand dollars ($2,000).
- For a new or renewal production license, the department shall charge an annual license fee of:
- Fifteen thousand dollars ($15,000), if the producer will possess up to one hundred fifty cannabis plants;
- and an additional five thousand dollars ($5,000) for each additional fifty cannabis plants the producer will possess;
- Cannabis and HEMP CBD strains at ratio of; 1.5 thc (or lower) : 1 cbd (or higher) are not counted against patient/caregiver or LNPP allowable plant count.
- Clones and Cuttings provided to qualified patient / caregiver with a PPL by a LNPP’s are not counted against LNPP allowable plant count.
- provided, however, that the maximum fee charged for a new or renewal production license shall not exceed forty-five thousand dollars ($45,000) per LNPP. The annual license fees provided for in this section are nonrefundable and shall be paid by upon the issuance of a license.
- Any resulting legalization of cannabis for adult recreational in the state of New Mexico, shall use a licensing fee structure; respectively, $4000 Annual Lic/$30,000 Production Lic/$7,500 per additional fifty cannabis plants.
- 7.10 percent of recreational cannabis sales are returned into the medical cannabis program to maintain and improve the program
- Licensure Limit Established: LNPP 1 Grow Location : 3 Store Fronts
- Current producers granted additional license per application review and program standards met
- Time Period for new producers to open; 90-120 (window) days Expected / Letter sent given final 45 days before forfeiture of license.
- The Department of Health shall employ 3 staff members to provide medical cannabis health education statewide. The Department of Health shall also establish a training or certification program for dispensary employees.
Lynn & Erin Compassionate Use Act Patient’s Coalition of New Mexico ~ A GrassRoots Movement!
UNITE-NETWORK-GROW-INFORM-KNOW-EDUCATE-ACTIVISM-VOTE-HEALTH-WELLNESS
(All Rights Reserved 04/20/2016)
No comments:
Post a Comment