

Saturday, September 16th 2017
New Mexico State Department of Health
Medical Cannabis Advisory Board
Medical Cannabis Program
PO Box 26110
Santa Fe, NM, 87502-6110
Medical Cannabis Program
PO Box 26110
Santa Fe, NM, 87502-6110
Petition: Requesting The Inclusion Of A New Medical Condition: Seizures; To Include The Two Main Types of Seizures: Focal Seizures And Generalized Seizures
(psychogenic neurologic disorders; Motor Disorders / Motor Development Disorders;In Addition to the twelve types of Epilepsy, which is currently part of the MCP)
(psychogenic neurologic disorders; Motor Disorders / Motor Development Disorders;In Addition to the twelve types of Epilepsy, which is currently part of the MCP)
Table of Contents
Pg. 1 Cover Page
Pg. 2 Petition Introduction
Pg. 3 Petition Purpose and Background
Pg. 15 Relief Requested In Petition
Pg. 15 References
Pg. 20-22 Appendix A
Petition Introduction:Requesting The Inclusion Of A New Medical Condition: Seizures; To Include The Two Main Types of Seizures: Focal Seizures And Generalized Seizures
New Mexico’s medical cannabis history started in 1978, after public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis. The New Mexico’s medical cannabis program (MCP) is the only program in the U.S. that places sole responsibility for regulation on the state’s Department of Health. Doctors must comply with state requirements for patients to be considered for applying to the medical cannabis program.
In the Lynn and Erin Compassionate Use Act, (2007) the law states; The Secretary of Health shall establish an advisory board consisting of eight practitioners representing the fields of neurology, pain management, medical oncology, psychiatry, infectious disease, family medicine and gynecology. The practitioners shall be nationally board-certified in their area of specialty and knowledgeable about the medical use of cannabis. The members shall be chosen for appointment by the Secretary from a list proposed by the New Mexico Medical Society. A quorum of the advisory board shall consist of three members. The advisory board shall:
A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis;
B. accept and review petitions to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
C. convene at least twice per year to conduct public hearings and to evaluate petitions, which shall be maintained as confidential personal health information, to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
D. issue recommendations concerning rules to be promulgated for the issuance of the registry identification cards; and
E. recommend quantities of cannabis that are necessary to constitute an adequate supply for qualified patients and primary caregivers.
First, do no harm. As an important step in becoming a doctor, medical students must take the Hippocratic Oath. And one of the promises within that oath is “first, do no harm”.
A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis;
B. accept and review petitions to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
C. convene at least twice per year to conduct public hearings and to evaluate petitions, which shall be maintained as confidential personal health information, to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
D. issue recommendations concerning rules to be promulgated for the issuance of the registry identification cards; and
E. recommend quantities of cannabis that are necessary to constitute an adequate supply for qualified patients and primary caregivers.
First, do no harm. As an important step in becoming a doctor, medical students must take the Hippocratic Oath. And one of the promises within that oath is “first, do no harm”.
We have a sound law in the Lynn and Erin Compassionate Use Act, as Section 2 reads; PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
“ARTICLE 2B. LYNN AND ERIN COMPASSIONATE USE ACT
N.M. Stat. Ann. § 26-2B-2 (2009)
§ 26-2B-2. Purpose of act
The purpose of the Lynn and Erin Compassionate Use Act [26-2B-1 NMSA 1978] is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
HISTORY: Laws 2007, ch. 210, § 2.
EFFECTIVE DATES. --Laws 2007, ch. 210, § 12 makes the act effective July 1, 2007.”
Mosby’s Medical Dictionary states that “medical treatment” means; the management and care of a patient to combat disease or disorder. Medical treatment includes: Using prescription medications, or use of a non-prescription drug at prescription strength; and or treatment of disease by hygienic and pharmacologic remedies, as distinguished from invasive surgical procedures. Treatment may be pharmacologic, using drugs; surgical, involving operative procedures; or supportive, building the patient's strength. It may be specific for the disorder, or symptomatic to relieve symptoms without effecting a cure.(Mosby's Medical Dictionary, 9th edition.)
What is a chronic medical condition?
A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear. Harvard Medical Dictionary defines chronic as: Any condition that lasts a long time or recurs over time; chronic pain as: Pain that persists after an injury has healed or a disease is over; and chronic pain syndrome as : Long-term, severe pain that doesn't spring from an injury or illness, that interferes with daily life, and is often accompanied by other problems, such as depression, irritability, and anxiety.
A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear. Harvard Medical Dictionary defines chronic as: Any condition that lasts a long time or recurs over time; chronic pain as: Pain that persists after an injury has healed or a disease is over; and chronic pain syndrome as : Long-term, severe pain that doesn't spring from an injury or illness, that interferes with daily life, and is often accompanied by other problems, such as depression, irritability, and anxiety.
What is the meaning of debilitating?
Something that's debilitating seriously affects someone or something's strength or ability to carry on with regular activities, like a debilitating illness. Debilitating comes from the Latin word debilis, meaning "weak." That's why you'll often see the adjective used to describe illness, despite the negative reference.
Something that's debilitating seriously affects someone or something's strength or ability to carry on with regular activities, like a debilitating illness. Debilitating comes from the Latin word debilis, meaning "weak." That's why you'll often see the adjective used to describe illness, despite the negative reference.
Petition Purpose and Background
The purpose of this Petition: Requesting The Inclusion Of A New Medical Condition: Seizures
This Petition: Requesting The Inclusion Of A New Medical Condition: Seizures; To Include The Two Main Types of Seizures: Focal Seizures And Generalized Seizures (In Addition to the twelve types of Epilepsy, which is currently part of the MCP) is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
Epilepsy is a brain disorder that happens when certain nerve cells in your brain misfire. It causes seizures, which can affect your behavior or the way you see things around you for a short time.
There are about a dozen to 20 different types of epilepsy, and the type you have plays a role in which kind of seizure you may have. (According to the Epilepsy Foundation)
Focal seizures: These start in a particular part of your brain, and their names are based on the part where they happen. They can cause both physical and emotional effects and make you feel, see, or hear things that aren’t there. About 60% of people with epilepsy have this type of seizure, which is sometimes called a partial seizure. Sometimes, the symptoms of a focal seizure can be mistaken for signs of mental illness or another kind of nerve disorder.
Generalized seizures: These happen when nerve cells on both sides of your brain misfire. They can make you have muscle spasms, black out, or fall.
Seizures aren’t always an either-or thing: Some people have seizures that start as one kind, then become another. And it’s not easy to classify some of them: These are called unknown-onset seizures, and they can cause both sensory and physical symptoms.
Generalized Seizures
There are six types:
Tonic-clonic (or grand mal) seizures: These are the most noticeable. When you have this type, your body stiffens, jerks, and shakes, and you lose consciousness. Sometimes you lose control of your bladder or bowels. They usually last 1 to 3 minutes -- if they go on longer, someone should call 911. That can lead to breathing problems or make you bite your tongue or cheek.
Clonic seizures: Your muscles have spasms, which often make your face, neck, and arm muscles jerk rhythmically. They may last several minutes.
Tonic seizures: The muscles in your arms, legs, or trunk tense up. These usually last less than 20 seconds and often happen when you’re asleep. But if you’re standing up at the time, you can lose your balance and fall. These are more common in people who have a type of epilepsy known as Lennox-Gastaut syndrome, though people with other types can have them, too.
Atonic seizures: Your muscles suddenly go limp, and your head may lean forward. If you’re holding something, you might drop it, and if you’re standing, you might fall. These usually last less than 15 seconds, but some people have several in a row. Because of the risk of falling, people who tend to have atonic seizures may need to wear something like a helmet to protect their heads.
People who have Lennox-Gastaut syndrome and another kind of epilepsy called Dravet syndrome are more likely to have this kind of seizure.
Myoclonic seizures: Your muscles suddenly jerk as if you’ve been shocked. They may start in the same part of the brain as an atonic seizure, and some people have both myoclonic and atonic seizures.
Absence (or petit mal) seizures: You seem disconnected from others around you and don’t respond to them. You may stare blankly into space, and your eyes might roll back in your head. They usually last only a few seconds, and you may not remember having one. They’re most common in children under 14.
Focal Seizures
Doctors break these into three groups:
Simple focal seizures: They change how your senses read the world around you: They can make you smell or taste something strange, and may make your fingers, arms, or legs twitch. You also might see flashes of light or feel dizzy. You’re not likely to lose consciousness, but you might feel sweaty or nauseated.
Complex focal seizures: These usually happen in the part of your brain that controls emotion and memory. You may lose consciousness but still look like you’re awake, or you may do things like gag, smack your lips, laugh, or cry. It may take several minutes for someone who’s having a complex focal seizure to come out of it.
Secondary generalized seizures: These start in one part of your brain and spread to the nerve cells on both sides. They can cause some of the same physical symptoms as a generalized seizure, like convulsions or muscle slackness.
RECENT STUDIES ON CANNABIS’ EFFECT ON SEIZURES
A cutting edge paper from three physicians—Dustin Sulak, Russel Saneto, and Bonni Goldstein—outlines case reports and the applications of cannabis medicine for epilepsy and seizure disorders.
Three physicians present promising data on artisanal cannabis, seizures, and epilepsy
Highlights:
- Physicians have documented the efficacy of artisanal whole plant cannabis preparations for seizure reduction.
- In a study of 272 patients, 86% had some degree of seizure reduction while using artisanal cannabis.
- A combination of cannabinoids and terpenes — not just CBD — may be most effective for seizures.
- These clinical findings challenge Big Pharma assumptions that favor single-molecule medications.
Cannabis clinicians treating epileptic patients in three medical marijuana states—California, Washington and Maine—have reported their findings in a peer-reviewed article that underscores the complex challenges and unique therapeutic potential of cannabis oil concentrates. In this uncontrolled observational study involving 272 patients, some degree of seizure reduction was noted in 86 percent of cases. Ten percent (26 patients) experienced complete seizure remission.
In addition to documenting the efficacy of “artisanal” (meaning not FDA-approved) cannabis preparations for seizure reduction, the article highlights the need for flexible treatment protocols involving different cannabinoid ratios, an approach that implicitly calls into question single-molecule strategies favored by Big Pharma.
What follows are excerpts from “The current status of artisanal cannabis for the treatment of epilepsy in the United States,” by Dustin Sulak, Russell Saneto, and Bonni Goldstein in the journal Epilepsy &Behavior:
Of 272 combined patients from Washington state and California, 37 (14 percent) found cannabis ineffective at reducing seizures, 29 (17 percent) experienced a 1-25 percent reduction in seizures, 60 (18 percent) experienced a 26-50 percent reduction in seizures, 45 (17 percent) experienced a 51-75 percent reduction in seizures, 75 (28 percent) experienced a 76-99 percent reduction in seizures and 26 (10 percent) experienced a complete clinical response. Overall, adverse effects were mild and infrequent, and beneficial side effects such as increased alertness were reported. The majority of patients used cannabidiol (CBD)-enriched artisanal formulas, some with the addition of delta-9-tetrahydrocannabinol (THC) and tetrahydrocannabinolic acid (THCA).
The authors maintain that artisanal cannabis products should be considered for patients with refractory epilepsy that have a low likelihood of responding to FDA-approved anti-epileptic drugs. Moreover, a combination of cannabinoid compounds—not just CBD—may be more effective for seizure reduction.
The patient population that considers herbal cannabis as a treatment for epilepsy is heterogeneous in etiology, currently predominantly pediatric, and has seizures that are usually refractory to multiple conventional treatments… The cannabinoids may reduce seizures via numerous mechanisms of action that warrant further investigation, including THC’s reduction of glutamate exotoxicity via the CB1 receptor, CBD’s modulation of numerous non-cannabinoid receptors, and several proposed targets of THCA. Objective measurement of treatment response can be challenging, and subjective reports of the efficacy of artisanal cannabis can be strongly influenced by the placebo effect, especially in patients that have invested significant resources into securing access to these formulas.
Several other challenges are cited by the authors:
Availability of a consistent supply of the medication is frequently interrupted due to horticultural, manufacturing, and economic factors. Current market prices for artisanal cannabis preparations observed in Maine, California, and online range from 5 to 50 cents per milligram. Higher dosing ranges are financially unfeasible for many patients unless they grow and produce their own medicine, a complex process that presents many potential interruptions in treatment. Sudden loss of access to cannabinoids may result in rebound seizures… The potential for disruption of medical treatment or family structure related to child protective services and other legal agencies, even when the patient and medical provider operate within state laws, must also be carefully considered on a case-by-case basis.
There are also serious issues of quality control with respect to artisanal cannabis preparations used by epilepsy patients.
[I]naccurate product labeling is pervasive in this new and often-unregulated industry. A 2015 study of edible cannabis products available in Seattle, San Francisco, and Los Angeles found that of 75 products examined, 17 percent were accurately labeled for cannabinoid content, 23 percent were inaccurate with higher than labeled concentrations, and 60 percent contained lower than labeled concentrations… Many patients purchase and use purportedly CBD-dominant “hemp” formulas that are sold online and shipped across state and international borders. Patients are led to believe that such products are legal, even in states without medical cannabis laws, despite the fact that CBD remains classified as Schedule One. In 2015 and again in 2016, the FDA published analytical results of several commercial CBD products and issued warning letters to their manufacturers. Many products were underlabeled for CBD content, contained no CBD, or contained significant amounts of THC.
The authors reference the ongoing clinical trials of Epidiolex, a CBD isolate developed by GW Pharmaceuticals, which has been evaluated at a dosing range of 2-50 mg/kg/day. Artisanal cannabis preparations have a wider therapeutic window than Epidiolex and are safe and effective at various dosages in clinical practice.
One of the authors [Dustin Sulak] has observed anticonvulsive effects in patients at doses as low as 0.02 mg cannabinoids per kilogram per day… Ultra-low doses of cannabinoids have been shown to be physiologically active in preclinical models: a single application of 0.002 milligrams per kilogram of THC to mice induced long lasting activation of protective signaling in molecules in the brain….
Cannabinoids trigger biphasic responses depending on dosage. Low doses and high doses can elicit opposite effects and this should not be unexpected in clinical practice. The authors comment on the clinical implications of potential biphasic dose-response trends in the anticonvulsant of activity of THC, CBD, and other modulators of the endocannabinoid system.
The extraordinarily wide dosing range of cannabis is complicated by non-linear dose-response relationships…. Clinicians are cautioned to avoid making the simple assumption that higher doses of cannabinoids will yield stronger therapeutic effects. If previous clinical improvements begin to diminish, especially after a dosage increase, clinicians may consider dosage reduction as a potential strategy to improve efficacy.
The authors also discuss the use of tetrahydrocannabinolic acid (THCA) for seizure reduction.
Delta-9-THC acid is becoming a popular treatment approach for patients with epilepsy in legal states, and is sometimes more readily available and/or affordable than CBD. THCA does not produce psychoactive effects in animals at relatively high doses, and psychoactivity has not been observed in humans. Though most THCA-dominant preparations will contain at least trace amounts of THC, THCA does not convert into THC in vivo.
In one case, THCA-rich therapy proved effective when treatment with CBD and THC failed to deliver satisfactory results. Specific terpenes, such as linalool (present in lavender and various cannabis cultivars), may also confer anticonvulsant effects.
Low-dose CBD at 0.05 mg/kg/day reportedly improved cognition, but higher doses of CBD caused an increase in myoclonic seizures. THC at 1 mg/kg/day reportedly produced a 4-day seizure-free episode, followed by recurrence of seizures. At 2 mg/kg/ day, THCA resulted in a reported overall 90 percent seizure reduction and improved tolerance to temperature fluctuations…. At one point a new formula of THCA at the same dosage resulted in notably decreased efficacy. A terpenoid analysis of the previous formula demonstrated the presence of high levels of alpha-linalool, absent in the less effective formula. Returning to a THCA formula based on the linalool-dominant chemovar improved her response.
Whereas pharmaceutical companies focus on single-molecule compounds, clinical practice indicates that medical marijuana patients with seizure disorders are more likely to benefit if they have access to a range of whole plant artisanal cannabis preparations, not just CBD.
Read the complete report at: https://www.projectcbd.org/sites/projectcbd/files/downloads/the_current_status_of_artisanal_cannabis_for_the_treatment_of_epilepsy_in_the_united_states.pdf
Seizures vs. Epilepsy
The medical definition of a seizure is a clinical expression of abnormal, excessive, synchronous discharge of neurons residing primarily in the brain’s cerebral cortex. Alternatively, the term epilepsy encompasses a broad range clinical syndromes characterized by repeated seizures over time unprovoked by an acute systemic or neurological insult.
The medical definition of a seizure is a clinical expression of abnormal, excessive, synchronous discharge of neurons residing primarily in the brain’s cerebral cortex. Alternatively, the term epilepsy encompasses a broad range clinical syndromes characterized by repeated seizures over time unprovoked by an acute systemic or neurological insult.
These definitions however fail to capture the feelings of helplessness felt by parents, family members, and caregivers when they watch a loved one endure the experience of a having a seizure – especially when that loved one is a child.
“It’s the last thing you worry about before you go to bed; and the first thing you think about when you wake up in the morning,” says Heather Jackson, Executive Director of Realm of Caring and mother to a child with an epilepsy syndrome.
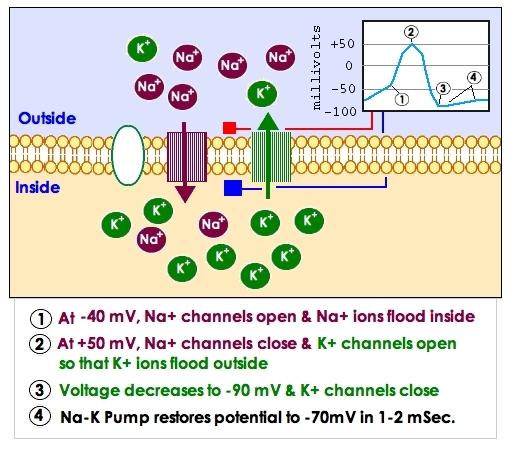
Under normal physiological conditions, the brain works by sending electrical signals through the nerves, which coordinate all of the functions of the body. These nerve impulses, are generated through a physiological process called an action potential. A simplified way to understand the concept of action potentials, is to view each nerve cell, or neuron, as electrically polarized. That is, there is an electrical difference between the inside and outside of a cell, created by the relative movement of the ions sodium (Na+) and potassium (K+).
This difference is maintained by the cell membrane which surrounds each cell. Neurons receive stimuli from other neurons in the area via neurotransmitters – chemicals that regulate brain function. This stimulation causes the polarity within each neuron to move towards a point which would cause the neuron to fire. Once a neuron has received so much stimulation that its polarity has reached the threshold point, an action potential is generated. This process is highly regulated under normal conditions.
In a seizure, regulatory control of action potentials is lost, and a synchronized burst of action potentials occur in a particular region of the brain due to a massive shift of Na+ ions into the cells in that region. This burst of action potentials activates surrounding neurons, causing them to fire and spread the seizure activity throughout the brain.
Types Of Seizures
Broadly, seizures are categorized by whether they are focal or generalized. Generalized seizures are further categorized according to their effect on the body; the categories are as follows:
- Tonic-clonic: also known as grand mal seizures, this seizure type is most associated with epilepsy. As the name suggests, it is comprised of two components. It begins with a tonic phase where an individual loses consciousness and muscles suddenly tense. After this short phase comes the clonic phase in which an individual’s muscles rapidly contract and relax. Confusion and short term amnesia usually follow these seizures.
- Absence: also known as petit mal seizures, this seizeure type varies significantly among patients. However, the general feature of absence seizures is an abrupt and sudden impairment of consciousness. During these seizures, activity is interrupted, speech is slowed or interrupted, and the individual becomes unresponsive. These seizures last from a few seconds to a minute and are not followed by confusion or lethargy.
- Myoclonic: colloquially known as jumps or jerks, these seizure types are characterized by rapid contraction and relaxation of muscles in multiple areas of the body.
- Atonic: also known as drops or akinetic seizures, atonic seizures are characterized by a brief lapse in muscles tone usually lasting less than fifteen seconds. A high risk of falling is associated with these seizures.
Epilepsy Syndromes
Individuals with epilepsy can manifest any of the above seizure types as part of their clinical condition. In fact, the International League Against Epilepsy recognizes over twenty epilepsy syndromes, each defined by a distinct set of signs and symptoms.
It is important to note that most epilepsy syndromes are extremely rare, with the prevalence in the US population ranging from 6-10/1000 individuals. However, the experience for patients with these disorders and their family members is quite significant. In children, many epilepsy syndromes have a strong genetic component, including benign familial infantile epilepsy, severe myoclonic epilepsy of infancy (Dravet syndrome), and Landau-Kleffner syndrome.
“Patients with this syndrome have a high propensity to enter into a life threatening state of status epilepticus, where the brain is in a persistent state of seizure.”
Perhaps the most notable and devastating of these syndromes, Dravet Syndrome, is a severe and intractable epilepsy condition. It presents in the first year of life as a series of prolonged generalized clonic seizures in the setting of otherwise normal cognitive and motor development.
Patients with this syndrome have a high propensity to enter into a life threatening state of status epilepticus, where the brain is in a persistent state of seizure. Unfortunately, children with this syndrome develop persistent gait ataxia – the inability to coordinate walking – in addition to cognitive and behavioral impairments.
Traditional Treatment Options
Treatment of epilepsy syndromes is a complex process involving a combination of drug therapy, diet, and even surgical intervention for some intractable cases. Antiepileptic drugs (AED) are administered according to the seizure type which is being treated. Additional factors such as side effect profile, cost, and method of administration are also highly considered, especially in the case of children.
While undergoing AED therapy, children will have to have their blood levels closely monitored in order to ensure that drug levels remain in the appropriate range – toxic levels of some AEDs may initiate seizure activity themselves. Patients and caregivers are very familiar with having to slowly increase the dosage of their medication to reach a maintenance dose which will provide optimal seizure control.

In 20-40% of children with epilepsy syndromes, lack of efficacy and side effects lead to the addition of a second AED to the therapeutic regimen. This further complicates treatment therapy however, as drug interactions and adverse interactions (ex. the induction of new seizure types) become a greater possibility once a second AED is introduced.
Additional options for those who have intractable seizures include consuming a ketogenic diet, which is a diet high in fat and protein and low in carbohydrates. The theoretical basis for this diet stems from the physiological principle that the brain has two sources of fuel: glucose and ketone bodies.
By significantly reducing the amount of carbohydrates in the diet, the brain will use ketone bodies as its primary fuel source which lowers the seizure threshold in patients. A meta-analysis of the efficacy of the ketogenic diet showed that after 6 months on the diet, approximately 60% of children had a greater than 50% seizure reduction, with 30% of children having greater than 90% seizure reduction.
Epilepsy Patients Turning Towards Cannabis Therapy
Unfortunately, multiple forms of AED therapy, switching to a ketogenic diet, and surgical intervention have failed to provide adequate seizure control for some epileptic children. It is for these patients and caregivers that medical cannabis therapy has provided a renewed sense of hope; but it is a decision that isn’t taken lightly.
“I never ran any of the pharmaceutical options by my family members, but I felt obligated to do so when we were considering cannabis therapy.” – Heather Jackson
“I never ran any of the pharmaceutical options by my family members, but I felt obligated to do so when we were considering cannabis therapy,” says Heather Jackson.
As Executive Director of Realm of Caring, breeders of the now famous Charlotte’s Web strain, Jackson is a strong advocate for cannabis therapy while managing expectations. “This isn’t a cure but it’s an option, an option that shouldn’t be relegated to an underground market,” she explains.
It seems that many lawmakers across the country are starting to agree with Jackson, as 11 states now having CBD-only legislation on their books – this is in addition to the 20+ states which have broader medical marijuana laws. “Unfortunately we have a lot of families who have to relocate, hopefully that won’t be an issue much longer,” says Jackson.
The Role Of Cannabis Therapy In Treating Epilepsy
The science of cannabis therapy in treating epilepsy is still in its infancy, but results have been promising. Historically, the English neurologists Drs. Russell Reynolds and William Gowers used cannabis Indica in conjunction with bromide as a therapy for epilepsy in the late 19th century.
In more modern preclinical animal studies conducted in the 1970s, CBD was shown to have anticonvulsant effects when seizures were acutely induced in mice. Later studies revealed a potential mechanism for this effect, showing that CBD raised the threshold requirement after one action potential, making it more difficult for subsequent action potentials to fire and propagate seizure activity. In humans, CBD has passed through the required safety and pharmacology trials, with very few issues or concerns. The cannabinoid is well tolerated and has no significant side effects or adverse reactions, which certainly cannot be said of AEDs.
Given these results, GW Pharmaceuticals was given the go ahead to conduct preliminary phase 3 clinical trials with their drug Epidiolex in select hospitals in the US under the FDA’s expanded access Investigational New Drugs (IND) program. Initial results have proved promising with an overall 44% seizure reduction seen in the 27 Dravet syndrome patients tested. Epidiolex is an investigational drug which comes in liquid form and contains 98% CBD, trace quantities of some other cannabinoids, and no THC. In spite of the promise of this drug, it will be years before the drug is available to the approximately 466,000 patients who could benefit from it.
“Out of 200 children treated at Realm of Caring, 78% have seen seizure reduction with 25% being almost 100% seizure free.”
In addition to undergoing three separate tests for purity, potential contaminants, the Charlotte’s Web extract is tested for its cannabinoid content – the cannabinoid profile is approximately 28:1 CBD to THC. Patients are started at 0.5mg/lb, and slowly increase the dose up until seizure control is established.
Out of 200 children treated at Realm of Caring, 78% have seen seizure reduction with 25% being almost 100% seizure free. Furthermore, Jackson reports, “Even if they don’t see the significant seizure control there are developmental gains.”
Realm of Caring has also been providing a strain of cannabis high in THCA for patients who have failed the CBD-rich treatment, and has seen some success here as well. As Jackson importantly points out, “These are very intractable cases, patients on average have tried at least 12 different therapies prior to cannabis, moreover, the safety profile is like night and day.”
In spite of the success, Jackson reports that the work of Realm of Caring is still an uphill battle “The epilepsy community much like cannabis has an unfair stigma.” Hopefully, the continued education and lobbying of policy makers by caring parents will move public understanding and acceptance of both epilepsy and cannabis therapy into the mainstream.
Does medical cannabis help seizures?
Evidence from laboratory studies, anecdotal reports, and small clinical studies from a number of years ago suggest that cannabidiol, a non-psychoactive compound of cannabis, could potentially be helpful in controlling seizures. Conducting studies can be difficult as researchers have limited access to marijuana due to federal regulations and even more limited access to cannabidiol; there are also increased financial and time constraints.
Cannabidiol (CBD)
Open-label studies in the U.S. of Epidiolex (a drug derived from cannabidiol or CBD) are being performed. Epidiolex is a purified, 99% oil-based CBD extract from the cannabis plant and is produced by GW Pharmaceuticals to give known and consistent amounts in each dose. The U.S. Food and Drug Administration (FDA) has given some epilepsy centers permission to use this drug as "compassionate use" for a limited number of people at each center.
Recently, gold-standard studies (double-blind, placebo-controlled studies) have finished for difficult epilepsies such as Lennox-Gastaut syndrome (LGS) in children and adults and Dravet syndrome in children. Information from these studies has been presented at major scientific meetings and in press releases by GW Pharmaceuticals.
Results from 214 people who received Epidiolex (99% CBD) in an open-label study (without a placebo control) and who completed 12 weeks or more on the drug were published in Lancet Neurology1.
- People who received Epidiolex ranged from 2 to 26 years old with an average age of 11.
- All had epilepsy that did not respond to currently available treatments.
- During the study, seizures decreased by an average of 54%.
- People taking the anti-seizure medication clobazam (Onfi) seemed to have a better response when compared to those that were not on this medication.
In addition, two gold-standard studies using Epidiolex for LGS in children and adults and one with children who have Dravet syndrome showed promising results.
- Drop seizures were reduced in the two LGS studies by over 40% compared to less than 20% for people who got the placebo, which was statistically significant.
- In the Dravet study, approximately 40% reduction in convulsive seizures was noted compared to 17% reduction for the placebo group. Again, significance was found compared to the placebo group.
An Israeli study2 using a product that had 20 parts of CBD to 1 part of THC was performed in an open-label format for children up to age 18 years with hard to control epilepsy. A significant number of people reported seizure reduction with 7% stating seizures worsened.
Safety of Medical Marijuana and Cannabis Products
Epilepsy Foundation - Uploaded on Jan 14, 2015 - https://youtu.be/7ygfHxrtkYw
Cannabinoids, Seizures and Research
The Cannabis plant offers a number of different cannabinoids, all of which have been found to have unique medicinal properties. The primary cannabinoid that gets the most attention is THC (Delta-9 Tetrahydrocannabinol). THC is the cannabinoid that is well known for being psychoactive. THC was also what lead scientists to discover the Endocannabinoid system in vertebrate animals, including humans (Steep Hill Laboratories, 2014). In one study from the 1940’s five children with “severe anticonvulsant resistant grand mal epilepsy” were treated with THC and found that THC controlled two of these children’s seizures. The other three children noted no change (Whalley, 2014). Additionally, there were several documented cases in a report by Lorenz (2004) in addition to the numerous preclinical studies conducted on animals. Many of the animal studies document successful control of seizures with THC.
Cannabidiol, otherwise known as CBD, is the only other cannabinoid that has been examined for anti-convulsant properties in humans. In 1978 two scientists conducted a randomized experiment on nine epileptic patients. Four of the patients were administered 200 mg of CBD daily. The remaining five patients were administered a placebo. Two of the four patients who received the 200 mg/daily dosage of CBD became seizure free (Whalley, 2014). There are further studies summarized in the paper by (Whalley) 2014, for a more in-depth examination of these studies follow this link: http://www.herbal-ahp.org/documents/press_releases/AHP%20Therapeutic%20Compendium-Cannabis%20Epilepsy%20and%20Seizures%20Scientific%20Review.pdf
A recent study of particular importance on CBD studies includes Porter and Jacobson (2013): they took a parent survey of cannabidiol enriched cannabis use in pediatric treatment-resistant epilepsy. The findings report: “The average number of antiepileptic drugs (AEDs) tried before using cannabidiol-enriched cannabis was 12. Sixteen (84%) of the 19 parents reported a reduction in their child’s seizure frequency while taking cannabidiol-enriched cannabis. Of these, two (11%) reported complete seizure freedom, eight (42%) reported a greater than 80% reductions in seizure frequency, and six (32%) reported a 25-60% seizure reduction. Other beneficial effects included increased alertness, better mood, and improved sleep. Side effects included drowsiness and fatigue. Our survey shows that parents are using cannabidiol-enriched cannabis as a treatment for their children with treatment-resistant epilepsy.” This study can be found at the following link: http://www.ncbi.nlm.nih.gov/pubmed/24237632 The overwhelming consensus of case studies, surveys and pre-clinical animal studies suggests CBD has a strong anticonvulsant effect; it has the potential to decrease or eliminate seizures, improve consciousness and spasticity.
Using Medical Cannabis as Medicine Safely For Seizures
The interaction between cannabinoids and each individual’s’ body is unique and complex. There is a wide variety in types of marijuana, each having its own unique cannabinoid and terpenoid make up. It is important to note that Cannabis has displayed both anti and pro convulsant properties. That said, in most human case studies cannabis tends to exert anticonvulsant properties. Due to the complex and varying interactions within each individual’s’ body, it is vital to track one’s experiences, particularly when a patient is new to using this medicine. We at Urban Farmacy suggest that you keep a journal of your experiences. Specifically, when you first start using cannabis or if you change the type of medicine you are using. You will find that each method of administering your medicine: sublingually, vaporizing, smoking or ingesting cannabinoids will elicit a different response in your mind and body. Furthermore, the strain of marijuana you choose and or the type of medicine you choose will also have variable effects on your condition and your body. When using cannabis as medicine we suggest that you continually educate yourself regarding cannabis strains, cannabinoids, terpenoids, and the endogenous cannabinoid system. The more knowledgeable you are, the wiser decisions you can make.
The next recommendation we have regarding using Cannabis as medicine is to start small and work up to a dosage that works best for your situation. Even in pharmacology, dosage varies by the person due to individual biochemistry. Since there are no established standards for dosing cannabis or cannabis extracts, you must carefully find what works for you. That said, there are case studies and anecdotal situations that can act as a guide as you navigate your way through experimenting with your dosages. Here is some key information when considering dosage for seizures:
1. “In the case of Charlotte Figi it was found that three to four milligrams of oil per pound of the girl’s body weight stopped the seizures” (Young, 2013).
2. This is the Mayo Clinic’s (2014) statement on dosage of CBD for seizures: “To treat epilepsy, 200-300 milligrams of CBD has been taken by mouth daily for up to 4.5 months.”
The following link is a summary of varying different cannabis and cannabinoid dosage used in scientific studies:
3. Finally, we encourage you to come by the shop or schedule a consultation to discuss any questions you may have. We have experience helping people find the right medicine and dosage for their conditions. We specifically have experience working with people to control their seizure disorders.
Austin’s Story
“Austin is 12 years old and has a rare and degenerative Mitochondrial Disease. Austin loves to tell jokes and make others laugh. He was having up to 200 seizures a month and slept the day away. His condition was deteriorating rapidly until we started working with Urban Farmacy. With the help of cannabis medicine Austin’s seizures have improved dramatically along with his energy level, mood and appetite.”-Sandy Roberts (Austin’s Mother)
Beneficial Cannabinoids and Terpenoids Useful for Treating Seizures
The cannabis plant offers a plethora of therapeutic benefits and contains cannabinoids and terpenoid compounds that are useful for treating the symptoms of all Seizures.
The following chart denotes which cannabinoids and terpenoids work synergistically with each other for potential therapeutic benefit. It may be beneficial to seek out strains that contain these cannabinoids and terpenoids.

Pediatric Seizures – Video Guide
A parent’s guide to understanding cannabis as a treatment for pediatric seizures. Dr. Dustin Sulak outlines what every parent considering cannabis as a seizure treatment for their child needs to understand in this video series. ( http://healer.com/pediatric-seizures-video-guide/)
A parent’s guide to understanding cannabis as a treatment for pediatric seizures. Dr. Dustin Sulak outlines what every parent considering cannabis as a seizure treatment for their child needs to understand in this video series. ( http://healer.com/pediatric-seizures-video-guide/)
Rules, Regulations, & Policy Solution For Requesting The Inclusion Of A New Medical Condition: Seizures
The approval of this petition: Requesting The Inclusion Of A New Medical Condition: Seizures; To Include The Two Main Types of Seizures: Focal Seizures And Generalized Seizures
(In Addition to the twelve types of Epilepsy, which is currently part of the MCP) that is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
(In Addition to the twelve types of Epilepsy, which is currently part of the MCP) that is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
The approval of this petition would bring the Department of Health in compliance with the intent of the law and uphold the spirit of the Lynn and Erin Compassionate Use Act, 2007. Fulfilling both;“ Section 2. PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments” And Section 6. ADVISORY BOARD CREATED--DUTIES: The advisory board shall: A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis.” New Mexico’s medical cannabis history started in 1978. After public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis...the first law.
References
Understanding medical cannabis.Elemental Wellness Center, 2014 Jul.
References I
- Devinsky O, Marsh E, Friedman D, et al. Cannabidiol in patients with treatment-resistant epilepsy: an open-label interventional trial. Lancet neurology 2015.
- Tzadok M, Uliel-Siboni S, Linder I, et al. CBD-enriched medical cannabis for intractable pediatric epilepsy: The current Israeli experience. Seizure : the journal of the British Epilepsy Association 2016;35:41-44.
- Gattone PM, Lammert W, and Devinsky O. Epilepsy Foundation of America Position Statement Medical Marijuana in Epilepsy [online].
- Devinksy O, Cilio MR, Cross H, et al. Cannabidiol: pharmacology and potential therapeutic role in epilepsy and other neuropsychiatric disorders. Epilepsia 2014.
Resources on Seizures and Cannabis:
Bienenstock, David. (2014). “Desperately Seeking CBD.” retrieved from: http://www.vice.com/read/desperately-seeking-cbd
Chaboya-Hembree, Jan. (2014). “Epilepsy – Can Medical Marijuana Aid in Relieving Seizures.” retrieved from: http://medicalmarijuana.com/experts/expert/title.cfm?artID=75
Lorenz R (2004) On the application of cannabis in pediatrics and epileptology Neuroendocrinology Letters 25:40-44
Lozano I (2001). The therapeutic use of Cannabis sativa L. in Arabic medicine. Journal of Cannabis Therapeutics 1(1): 63-70.
Porter, BE. Jacobson, C. (2013). “Report of a parent survey of cannabidiol-enriched cannabis use in pediatric treatment-resistant epilepsy.” retrieved from: http://www.ncbi.nlm.nih.gov/pubmed/24237632
Mayo Clinic. (2014). Marijuana (Cannabis Sativa): Dosage. retrieved from: http://www.mayoclinic.org/drugs-supplements/marijuana/dosing/hrb-20059701
University of Maryland Medical Center. (2014). “Seizure Disorders.” retrieved from: http://umm.edu/health/medical/altmed/condition/seizure-disorders
Schwartz, Carly. (2014). “Meet the Children Who Rely on Marijuana to Survive.” retrieved from:
Steep Hill Laboratories. (2014). Cannabinoid and Terpenoid Reference Guide. retrieved from: http://steephilllab.com/resources/cannabinoid-and-terpenoid-reference-guide/
Whalley, Benjamin J. (2014). “Cannabis In The Management And Treatment Of Seizures And Epilepsy: A Scientific Review.” American Herbal Pharmacopoeia.
retrieved from: http://www.herbal-ahp.org/documents/press_releases/AHP%20Therapeutic%20Compendium-Cannabis%20Epilepsy%20and%20Seizures%20Scientific%20Review.pdf
Young, Saundra. (2014). “Marijuana Stops Child’s Severe Seizures.” CNN. retrieved from: http://www.cnn.com/2013/08/07/health/charlotte-child-medical-marijuana/
Appendix A:
WHEREAS cannabis (marijuana) has been used as a medicine for at least 5,000 years and can be effective for serious medical conditions for which conventional medications fail to provide relief;
WHEREAS modern medical research has shown that cannabis can slow the progression of such serious diseases as Alzheimer’s and Parkinson’s and stop HIV and cancer cells from spreading; has both anti-inflammatory and pain-relieving properties; can alleviate the symptoms of epilepsy, PTSD and multiple sclerosis; is useful in the treatment of depression, anxiety and other mental disorders; and can help reverse neurological damage from brain injuries and stroke;
WHEREAS the World Health Organization has acknowledged the therapeutic effects of cannabinoids, the primary active compounds found in cannabis, including as an anti-depressant, appetite stimulant, anticonvulsant and anti-spasmodic, and identified cannabinoids as beneficial in the treatment of asthma, glaucoma, and nausea and vomiting related to illnesses such as cancer and AIDS;
WHEREAS the American Medical Association has called for the review of the classification of cannabis as a Schedule I controlled substance to allow for clinical research and the development of cannabinoid-based medicines;
WHEREAS the National Cancer Institute has concluded that cannabis has antiemetic effects and is beneficial for appetite stimulation, pain relief, and improved sleep among cancer patients;
WHEREAS the American Herbal Pharmacopoeia and the American Herbal Products Association have developed qualitative standards for the use of cannabis as a botanical medicine;
WHEREAS the U.S. Supreme Court has long noted that states may operate as “laboratories of democracy” in the development of innovative public policies;
WHEREAS twenty-eight states and the District of Columbia have enacted laws that allow for the medical use of cannabis;
WHEREAS seventeen additional states have enacted laws authorizing the medical use of therapeutic compounds extracted from the cannabis plant;
WHEREAS more than 17 years of state-level experimentation provides a guide for state and federal law and policy related to the medical use of cannabis;
WHEREAS accredited educational curricula concerning the medical use of cannabis have been established that meets Continuing Medical Education requirements for practicing physicians;
WHEREAS Congress has prohibited the federal Department of Justice from using funds to interfere with and prosecute those acting in compliance with their state medical cannabis laws, and the Department of Justice has issued guidance to U.S. Attorneys indicating that enforcement of the Controlled Substances Act is not a priority when individual patients and their care providers are in compliance with state law, and that federal prosecutors should defer to state and local enforcement so long as a viable state regulatory scheme is in place.
WHEREAS modern medical research has shown that cannabis can slow the progression of such serious diseases as Alzheimer’s and Parkinson’s and stop HIV and cancer cells from spreading; has both anti-inflammatory and pain-relieving properties; can alleviate the symptoms of epilepsy, PTSD and multiple sclerosis; is useful in the treatment of depression, anxiety and other mental disorders; and can help reverse neurological damage from brain injuries and stroke;
WHEREAS the World Health Organization has acknowledged the therapeutic effects of cannabinoids, the primary active compounds found in cannabis, including as an anti-depressant, appetite stimulant, anticonvulsant and anti-spasmodic, and identified cannabinoids as beneficial in the treatment of asthma, glaucoma, and nausea and vomiting related to illnesses such as cancer and AIDS;
WHEREAS the American Medical Association has called for the review of the classification of cannabis as a Schedule I controlled substance to allow for clinical research and the development of cannabinoid-based medicines;
WHEREAS the National Cancer Institute has concluded that cannabis has antiemetic effects and is beneficial for appetite stimulation, pain relief, and improved sleep among cancer patients;
WHEREAS the American Herbal Pharmacopoeia and the American Herbal Products Association have developed qualitative standards for the use of cannabis as a botanical medicine;
WHEREAS the U.S. Supreme Court has long noted that states may operate as “laboratories of democracy” in the development of innovative public policies;
WHEREAS twenty-eight states and the District of Columbia have enacted laws that allow for the medical use of cannabis;
WHEREAS seventeen additional states have enacted laws authorizing the medical use of therapeutic compounds extracted from the cannabis plant;
WHEREAS more than 17 years of state-level experimentation provides a guide for state and federal law and policy related to the medical use of cannabis;
WHEREAS accredited educational curricula concerning the medical use of cannabis have been established that meets Continuing Medical Education requirements for practicing physicians;
WHEREAS Congress has prohibited the federal Department of Justice from using funds to interfere with and prosecute those acting in compliance with their state medical cannabis laws, and the Department of Justice has issued guidance to U.S. Attorneys indicating that enforcement of the Controlled Substances Act is not a priority when individual patients and their care providers are in compliance with state law, and that federal prosecutors should defer to state and local enforcement so long as a viable state regulatory scheme is in place.
No comments:
Post a Comment