
Saturday, September 16th 2017
New Mexico State Department of Health
Medical Cannabis Advisory Board
Medical Cannabis Program
PO Box 26110
Santa Fe, NM, 87502-6110
Medical Cannabis Program
PO Box 26110
Santa Fe, NM, 87502-6110
Petition: Requesting The Inclusion Of A New Medical Treatment: Pediatric Oncology And Cannabis Use for Antiemetic In State Hospitals (department to create Rules and Regulations for medical cannabis use in hospitals in New Mexico for Pediatric Oncology And Cannabis Use for Antiemetic as the Lynn and Erin Compassionate Use Act does allow for)
Table of Contents
Pg. 1 Cover Page
Pg. 2 Petition Introduction
Pg. 3 Petition Purpose and Background
Pg. 21 Relief Requested In Petition
Pg. 21 References
Pg. 21-22 Appendix A
Petition: Requesting The Inclusion Of A New Medical Treatment: Pediatric Oncology And Cannabis Use for Antiemetic In State Hospitals
New Mexico’s medical cannabis history started in 1978, after public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis. The New Mexico’s medical cannabis program (MCP) is the only program in the U.S. that places sole responsibility for regulation on the state’s Department of Health. Doctors must comply with state requirements for patients to be considered for applying to the medical cannabis program.
In the Lynn and Erin Compassionate Use Act, (2007) the law states; The Secretary of Health shall establish an advisory board consisting of eight practitioners representing the fields of neurology, pain management, medical oncology, psychiatry, infectious disease, family medicine and gynecology. The practitioners shall be nationally board-certified in their area of specialty and knowledgeable about the medical use of cannabis. The members shall be chosen for appointment by the Secretary from a list proposed by the New Mexico Medical Society. A quorum of the advisory board shall consist of three members. The advisory board shall:
A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis;
B. accept and review petitions to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
C. convene at least twice per year to conduct public hearings and to evaluate petitions, which shall be maintained as confidential personal health information, to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
D. issue recommendations concerning rules to be promulgated for the issuance of the registry identification cards; and
E. recommend quantities of cannabis that are necessary to constitute an adequate supply for qualified patients and primary caregivers.
First, do no harm. As an important step in becoming a doctor, medical students must take the Hippocratic Oath. And one of the promises within that oath is “first, do no harm”.
A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis;
B. accept and review petitions to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
C. convene at least twice per year to conduct public hearings and to evaluate petitions, which shall be maintained as confidential personal health information, to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
D. issue recommendations concerning rules to be promulgated for the issuance of the registry identification cards; and
E. recommend quantities of cannabis that are necessary to constitute an adequate supply for qualified patients and primary caregivers.
First, do no harm. As an important step in becoming a doctor, medical students must take the Hippocratic Oath. And one of the promises within that oath is “first, do no harm”.
We have a sound law in the Lynn and Erin Compassionate Use Act, as Section 2 reads; PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
“ARTICLE 2B. LYNN AND ERIN COMPASSIONATE USE ACT
N.M. Stat. Ann. § 26-2B-2 (2009)
§ 26-2B-2. Purpose of act
The purpose of the Lynn and Erin Compassionate Use Act [26-2B-1 NMSA 1978] is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
HISTORY: Laws 2007, ch. 210, § 2.
EFFECTIVE DATES. --Laws 2007, ch. 210, § 12 makes the act effective July 1, 2007.”
Mosby’s Medical Dictionary states that “medical treatment” means; the management and care of a patient to combat disease or disorder. Medical treatment includes: Using prescription medications, or use of a non-prescription drug at prescription strength; and or treatment of disease by hygienic and pharmacologic remedies, as distinguished from invasive surgical procedures. Treatment may be pharmacologic, using drugs; surgical, involving operative procedures; or supportive, building the patient's strength. It may be specific for the disorder, or symptomatic to relieve symptoms without effecting a cure.(Mosby's Medical Dictionary, 9th edition.)
What is a chronic medical condition?
A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear. Harvard Medical Dictionary defines chronic as: Any condition that lasts a long time or recurs over time; chronic pain as: Pain that persists after an injury has healed or a disease is over; and chronic pain syndrome as : Long-term, severe pain that doesn't spring from an injury or illness, that interferes with daily life, and is often accompanied by other problems, such as depression, irritability, and anxiety.
A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear. Harvard Medical Dictionary defines chronic as: Any condition that lasts a long time or recurs over time; chronic pain as: Pain that persists after an injury has healed or a disease is over; and chronic pain syndrome as : Long-term, severe pain that doesn't spring from an injury or illness, that interferes with daily life, and is often accompanied by other problems, such as depression, irritability, and anxiety.
What is the meaning of debilitating?
Something that's debilitating seriously affects someone or something's strength or ability to carry on with regular activities, like a debilitating illness. Debilitating comes from the Latin word debilis, meaning "weak." That's why you'll often see the adjective used to describe illness, despite the negative reference.
Something that's debilitating seriously affects someone or something's strength or ability to carry on with regular activities, like a debilitating illness. Debilitating comes from the Latin word debilis, meaning "weak." That's why you'll often see the adjective used to describe illness, despite the negative reference.
Petition Purpose and Background
The purpose of this Petition: Requesting The Inclusion Of A New Medical Treatment: Pediatric Oncology And Cannabis Use for Antiemetic In State Hospitals (department to create Rules and Regulations for medical cannabis use in hospitals in New Mexico for Pediatric Oncology And Cannabis Use for Antiemetic as the Lynn and Erin Compassionate Use Act does allow for.)
This Petition: Requesting The Inclusion Of A New Medical Treatment: Pediatric Oncology And Cannabis Use for Antiemetic In State Hospitals is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
Who Should Qualify for Medical Cannabis Use?
According to Americans For Safe Access Policy Studies & Research:
Background: The most fundamental aspect of medical cannabis laws is the relationship between a patient and their physician. It is often only the physician and the patient that possess information about a patient’s health condition. However, many public officials and others who oppose medical cannabis laws often make assumptions about people’s health. The media have even fomented such inappropriate assumptions by naming a category of patients “Young Able Bodied Males,” condemning certain patients by visual assessment alone.
Findings: The health care information discussed between a patient and physician is considered private and protected under federal HIPAA laws. It is typically the purview of state medical boards to assess whether a physician has inappropriately recommended cannabis to someone who should not be qualified. Studies have shown in some medical cannabis states that the majority of patients suffer from chronic pain, an ailment that is not obviously detectable by another person. Nevertheless, police will often harass and arrest patients based on the assumption that someone is faking their illness.
Position: Medical professionals should have an unrestricted ability to recommend cannabis therapeutics and that should not be impacted by law enforcement’s perceptions.
According to Americans For Safe Access Policy Studies & Research:
Background: The most fundamental aspect of medical cannabis laws is the relationship between a patient and their physician. It is often only the physician and the patient that possess information about a patient’s health condition. However, many public officials and others who oppose medical cannabis laws often make assumptions about people’s health. The media have even fomented such inappropriate assumptions by naming a category of patients “Young Able Bodied Males,” condemning certain patients by visual assessment alone.
Findings: The health care information discussed between a patient and physician is considered private and protected under federal HIPAA laws. It is typically the purview of state medical boards to assess whether a physician has inappropriately recommended cannabis to someone who should not be qualified. Studies have shown in some medical cannabis states that the majority of patients suffer from chronic pain, an ailment that is not obviously detectable by another person. Nevertheless, police will often harass and arrest patients based on the assumption that someone is faking their illness.
Position: Medical professionals should have an unrestricted ability to recommend cannabis therapeutics and that should not be impacted by law enforcement’s perceptions.
“Qualifying medical condition” shall mean any condition for which treatment with medical cannabis would be beneficial, as determined by a patient's qualified medical professional, including but not limited to cancer, glaucoma, positive status for human immunodeficiency virus, acquired immune deficiency syndrome (AIDS), hepatitis C, amyotrophic lateral sclerosis (ALS), Crohn’s disease, Parkinson’s disease, post-traumatic stress disorder, arthritis, chronic pain, neuropathic and other intractable chronic pain, and multiple sclerosis.
“Qualifying patient” shall mean a person who has a written recommendation from a qualified medical professional for the medical use of cannabis.
A Look Back And Ahead: Cannabinoid Antiemetic In Pediatric Oncology

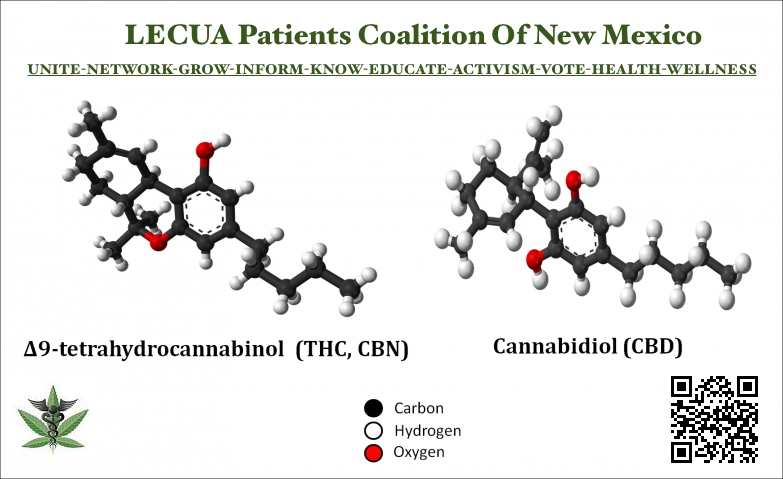
Cannabis is one of the first plants to have been used as a medicine, for religious ceremonies and recreationally, the first accounts of its use for these purposes stretching back over 5000 years. Modern research into the pharmacology of individual cannabinoids began in the 1940s, several decades after the presence of a cannabinoid was first discovered in cannabis. Cannabinol (CBN), much of which is thought to be formed from THC during the storage of harvested cannabis, was the first of the plant cannabinoids (phytocannabinoids) to be isolated in the early 1930s by R.S. Cahn, and its chemical synthesis first achieved in 1940 in the laboratories of R. Adams in the U.S. and Lord Todd in the U.K. A second phytocannabinoid, Cannabidiol (CBD), was first obtained from cannabis in the same year (1940) by Adams and his colleagues. It was in Prof. Raphael Mechoulam's laboratory, when the structures and chemistry of CBD (1963) and Δ9-THC (1964) mysteries are unravelled (Mechoulam, 1973; Mechoulam & Hanus, 2000).
Research into the therapeutic potential of cannabis and individual cannabinoids began in the 1970s, ironically at a time when tincture of cannabis had just been withdrawn as a medicine in the U.K. because at that time was the widespread recreational use of cannabis.
In 1995 Science Provides The Realization: Cannabis Helps Children Undergoing Cancer Treatment.

The number of hospitals in New Mexico using medical cannabis in pediatric oncology? Zero.
The number of hospitals in the United States using medical cannabis in pediatric oncology? Zero. Yet we always hear lawmakers and politicians talking about the importance of the children in our country - after all they are the future...
Oncology is the study of cancer. ... Usually, an oncologist manages a person's care and treatment once he or she is diagnosed with cancer. The field of oncology has three major areas: medical, surgical, and radiation. A medical oncologist treats cancer using chemotherapy or other medications, such as targeted therapy. And they typically have a median income of $320,907 a year where as a family physicians earned an average of $208,861 a year.
In 1995, The Scientist, Raphael Mechoulam (The Brettler Center for Medical Research, Medical Faculty, Hebrew University, Jerusalem) published a study with Dr. Aya Abrahamov (Department of Pediatrics, Shaare Zedek Hospital, Jerusalem, Israel) and Dr. Avraham Abrahamov (Department of Pediatrics, Bikur Holim Hospital, Jerusalem); An efficient new cannabinoid antiemetic in pediatric oncology. Journal of the International Hemp Association 2(2): 76-79.
Medical Cannabis, Children and Cancer Treatment: ‘Hashish For Children’

So in 1995 Dr. Mechoulam had an idea to test THC on children undergoing cancer treatments, as it had been known for many years that cannabis can reduce the effects of cancer drugs. Anti-cancer drugs, many of them cause terrible side effects for adults, for children this can be much worse. And in children, many of them vomit, have nausea, are crying from the pain - they’re in really bad shape. And this makes it a challenge for the parents of these children as this all take a toll on them as well. Luckily most of the children today can be cured of the cancer, but the treatment is absolutely beyond difficult. (Additional side effect of anticancer drug treatments include; Low blood counts causes an increased possibility of developing infection or anemia. Tiredness. Mouth soreness. Loss of appetite. Constipation or diarrhea. Hair loss. Skin changes or reactions.)
What Dr. Mechoulam wanted to do was a clinical trial in children. He did a major study with Dr. Aya Abrahamov (Department of Pediatrics, Shaare Zedek Hospital, Jerusalem, Israel) and Dr. Avraham Abrahamov (Department of Pediatrics, Bikur Holim Hospital, Jerusalem).
What they did for the study was give THC drops in olive oil under the tongue of children. Obviously, children cannot smoke, they had children that were not even one year old yet. Dr. Aya Abrahamov gave the children 2-3 drops of the THC infused Olive Oil, micro doses, 2-3 time per day during anti-cancer drug treatments. At the a start of the clinical trial, Dr. Mechoulam wanted to do a double-blind study where some of the children got THC Olive Oil and some got just Olive Oil.
After one week Dr. Aya Abrahamov came back to Dr. Mechoulam and she told him that she was not going ahead with the double-blind study. Dr. Aya Abrahamov then told Dr. Mechoulam, “I know exactly who is getting the THC and exactly who is not getting it.” There was a clear separation right from the get go, those didn’t get it continued to vomit, so she went ahead with an open study.
Dr. Aya Abrahamov gave the THC Olive Oil, pure THC, under the tongue about 400 times, which means that those in the experiment got the THC every time they were treated with the anticancer drugs. And by the end of the study they had seen a complete, complete block of vomiting, complete block of nausea, by a small amount of THC that did not cause any psychoactivity- none at all. So here we have a complete therapeutic effect proven that they published back in the 90’s .
Over 20 years later and this is still not being used in hospitals in New Mexico or across the US to alleviate terrible side effects of anticancer drugs. Allowing medical cannabis as a antiemetic in pediatric oncology for use in all hospitals is an excellent idea because it will help the children that suffer. It is scientifically and medically proven safe and effective. It is unethical to withhold this form of treatment.
“In summary, the complete success in preventing vomiting due to antineoplastic treatment in children, and the essential lack of side effects, leads us to believe that delta-8-THC at a dose considerably higher than the doses of delta-9-THC usually administered to adults, can serve as a new, inexpensive antiemetic agent in pediatric cancer chemotherapy.”
See below to review the research study:
An efficient new cannabinoid antiemetic in pediatric oncology
1 Department of Pediatrics, Shaare Zedek Hospital, Jerusalem, Israel;
2 Department of Pediatrics, Bikur Holim Hospital, Jerusalem;
3 The Brettler Center for Medical Research, Medical Faculty,
Hebrew University, Jerusalem 91120.
Abrahamov, Aya, Avraham Abrahamov, and R. Mechoulam, 1995. An efficient new cannabinoid antiemetic in pediatric oncology. Journal of the International Hemp Association 2(2): 76-79.
Delta-8-tetrahydrocannabinol (delta-8-THC), a cannabinoid with lower psychotropic potency than the main Cannabis constituent, delta-9-tetrahydrocannabinol (delta-9-THC), was administered (18 mg/m2 in edible oil, p.o.) to eight children, aged 3-13 years with various hematologic cancers, treated with different antineoplastic drugs for up to 8 months. The total number of treatments with delta-8-THC so far is 480. The THC treatment started two hours before each antineoplastic treatment and was continued every. 6 hrs for 24 hours. Vomiting was completely prevented. The side effects observed were negligible.
Introduction
Cannabis preparations have been used for millenia as antiemetic drugs [1]. With the identification of delta-9-tetra-hydrocannabinol (delta-9-THC) (Fig 1) as the psychoactive Cannabis constituent [2] its evaluation as an antivomiting agent was also made possible. It was indeed found that delta-9-THC prevents or reduces vomiting induced by anticancer chemotherapy [3-5]. Delta-9-THC is marketed under the generic name Dronabinol [5]. Depending on the clinical protocol used, delta-9-THC (5-10 mg/m2 p.o.) prevents vomiting and nausea in some patients and reduces these symptoms in others. The side effects are those noted in marijuana users, in particular elderly ones: drowsiness, dizziness and in rare cases anxiety. Mood changes usually predominate in younger patients.
DeIta-8-THC (Fig 1 ) is a double bond isomer of delta-9-THC. It is less psychotropic than delta-9-THC [6], but its antiemetic potential has not been investigated so far. In preclinical antiemetic studies in pigeons (to be reported separately), using the methodology previously described by us for delta-9-THC [7], we found that delta-8-THC is at least as potent as delta-9-THC. It is much more stable than delta-9-THC to various chemical treatments, including oxidation, and is considerably less expensive to produce than delta-9-THC. Hence. it seemed of potential therapeutic interest to investigate the antiemetic effect of delta-8-THC in patients. We chose to administer delta-8-THC to children, who were expected to vomit on anticancer chemotherapy. The reason for the age limitation was the general (but not documented) belief that most side effects of delta-9-THC, in particular anxiety, are more prevalant in an adult population than in a younger one. Hence delta-8-THC could possibly be administered to children in higher doses than those given to adult patients.
We report now that delta-8-THC in an open label evaluation was found to be an excellent pediatric antiemetic with nonsignificant side effects. We chose an open label trial for ethical reasons. A clinical trial based on placebo versus delta-8 THC as an antiemetic agent during anticancer treatment is unacceptable. Our original protocol envisaged a comparison between metoclopramide (0.3 mg/kg) and delta-8-THC (18 mg/m2). However preliminary results indicated complete block of emesis with delta-8-THC, while metoclopramide showed variable results. Most of the children (5 out of 8) vomited with this dose of metoclopramide. In higher doses (0.5 mg/kg dose or above) metoclopramide caused extrapyramidal effects. Hence for ethical reasons the protocol was modified to an open trial design. However, we would like to point out that over a period of about 10 years, when most of the antineoplastic protocols followed in the present study were used in our clinic, emesis was observed in about 60% of all pediatric cases even though metoclopramide (0.3 mg/kg) was used as antiemetic agent.
Ondansetrone and other HT3-receptor blockers are today the drugs of choice for chemotherapy-induced vomiting and nausea [8]. While such therapy is superior to previously used treatments (dopamine antagonists, corticosteroids) adverse effects such as headache are troublesome [8] and its efficiency in delayed vomiting is questionable. Ondansetrone is also a very expensive drug and less expensive alternatives should be made available. Hence additional therapeutic protocols are required.
Materials, patients and clinical protocol
Delta-8-THC was prepared from natural cannabidiol by cyclization (Figure 1) and purified by chromatography as previously described [9]. It was analyzed by gas chromatography and was found to be 98% pure.
Figure 1. Chemical structures of cannabinoid compounds
Eight children with various blood cancers (see Table) were administered delta-8-THC (18 mg/m2 p.o.) two hours before the start of the anticancer treatment. The drug was dissolved in corn or olive oil (6 mg/ml), and was administered directly as oil drops on the tongue, or on a bite of bread. The same dose was repeated every 6 hrs for 24 hrs. The treatment tor each child is presented in the Table. Whenever additional cycles of antineoplastic therapy were required, delta-8-THC was administered following the same time procedure described above. Children received delta-8-THC only during days when emetogenic drugs were administered. Established anticancer drug protocols were followed with all patients. These are indicated below and in Table 1:
High-dose Cytarabine and Asparaginase [10] (Patient 1) MOPP-ABV protocol [11] (Patient 2). This protocol is a standard combination of Mechlorethamine hydrochloride, Vincristine, Procarbazine, Prednisone, Doxorubicin, Bleomycin and Vinblastine. BFM protocol [12] (patients 3 and 8). This protocol is a complicated standard protocol consisting of numerous antineoplastic drugs (Vincristine, Daunorubicine, L-Asparaginase, Cyclophosphamide, Cytarabine, Mercaptopurine, Etoposide, Methotrexate, Thioguanine) and 3 types of corticosteroids (Prednisone, Hydrocortisone, Dexamethasone) in p.o., i.v. and intratecal administrations. National Wilm’s tumor study protocol (NWTS-4) [13] (Patient 4). This protocol is a standard combination of Vincristine, Doxorubicin, Dactinomycin. Amsacrine-high dose Cytarabine protocol [14] (Patient 5). This is a standard protocol consisting of Cytarabine and Amsacrine. Burkitt's lymphona protocol [15] (Patient 6). This is a standard protocol consisting of Vinscristine, Doxorubicin Cyclophosphamide, Methotrexate and Prednisone. Rezidive study. A.L.L. - Rez BFM 87 protocol [16] (Patient 7). This is a standard complicated protocol consisting of numerous antineoplastic drugs. In addition to drugs mentioned above it includes Ifosfamide and Vindesine.
Results
The present study on prevention of vomiting due to antineoplastic therapy took place over a 2 year period with 8 patients. Details of their antineoplastic treatment and side effects of the antiemetic therapy are presented in Table 1. The mild side effects observed were reported by the physician and nurse in charge. Chemotherapy protocols of the types indicated almost invariably cause intense vomiting, which starts about 2 hrs after the initiation of chemotherapy and gradually ends over a 24 hr period. In prelimary trials we tried to end the antiemetic therapy after the first or second dose of the cannabinoid, i.e. after 6 or 12 hrs. Vomiting started in most cases. Hence, in the recorded trial, all children were given 4 doses (every 6 hours) for 24 hrs. When the antiemetic protocol described in the "Methods, patients and clinical protocol" section was strictIy followed, no emesis was noted during the 24 hrs of treatment or over the next two days. In one case (patient D.E.), delta-8-THC therapy initially was refused. The patient experienced debilitating vomiting for 24 hrs after the antineoplastic treatment. During the second treatment cycle (which took place after 8 days), at the patient's family request, delta-8-THC treatment was initiated. No vomiting occurred. In a second case (A.M.), the patient refused antiemetic treatment during a relapse of his disease as it was based on an "illicit drug" (Cannabis). Repeated vomiting took place. Renewal of the THC treatment, before the next administration of antineoplastic drugs, prevented additional vomiting. As indicated in Table 1 the side effects were observed in only 2 of the 8 patients: some irritability and slight euphoria which in children is difficult to quantify. No anxiety or hallucinogenlc effects were noted in spite of the high doses administered.
No.
|
Name
sex
|
Age
(years)
|
Diagnostic treatmentc
|
Antineoplastic
|
Number and effect of antiemetic treatments
|
1.
|
A.M.
m
|
10
|
in relapse
|
Cytarabine-
L-Asparaginase
|
(32), no side effects
|
2.
|
C.O.
m
|
3.5
|
Hodgkin's
disease
|
MOPP-ABV
protocol
|
(64), slight irritability
dudng first 2 cycles
|
3.
|
L.H.
f
|
4
|
A.L.L.,
T type
|
BFM protocol
|
(76), slight irritability
and euphoria1
|
4.
|
M.H.
f
|
3
|
Wilm's tumor,
stage 1II
|
NWTS-4
protocol
|
(30), no side effects
|
5.
|
R.M.
f
|
13
|
A.L.L., T type
in second
relapse
|
Cytarabine,
Amsacrine
protocol
|
(24), no side effects
|
6.
|
DE.
m
|
7
|
Burkitt's
lymphoma
|
Burkitt's lymphoma
protocol
|
(114), no side effects2
|
7.
|
K.K.
f
|
6
|
A.L.L.
|
Rez BFM 87
protocol
|
(64), no side effects3
|
8.
|
A.A.
m
|
5
|
A.L.L.
|
BFM protocol
|
(76), no side effects
|
a Delta-8 THC, 18 mg/m2. For details see text. In all cases complete prevention of vomiting was noted.
b Acute Lymphoblastic Leukemia (A.L.L.). c see Methods, patients and clinical protocol.
| |||||
1 Metoclopromide (0.3 mg/kg) p.o. or i.v. in previous treatment failed to prevent vomiting.
2 During first cycle, refusal to take THC caused profuse vomiting.
3 Treatment during remission after 2nd relapse and during 3rd relapse.
| |||||
Discussion
Delta-8-THC is an isomer of delta-9-THC, the major natural constituent of Cannabis from which it differs only in the position of the double bond. The stereochemistry of the two isomers is identical; their chemical behavior is in most cases very similar [17]; their metabolism in vivo and in vitro follow the same pathways [18]. The major chemical difference between them is that delta-9-THC is easily oxidized to the biologically inactive cannabinol; delta-8-THC is stable, does not oxidize to cannabinol and has a very long shelf life. Due to their close structural similarity, delta-9-THC and delta-8-THC present essentially identical pharmacological profiles [19-21]. Quantitatively, however, delta-8-THC differs from delta-9-THC in being about twice less potent in most, but not all pharmacological tests.
In monkeys delta-8-THC causes a general behavior depression in doses reported to be higher than the doses of delta-9-THC required to produce similar effects [22, 23].
A direct comparison of the effects of delta-8-THC (20 and 40 mg total dose) and of delta-9-THC (20 mg total dose) orally administered to human volunteers has been published [24]. The spectrum of clinical effects was similar with both isomers, but delta-8-THC was considered to be only 3/4 as psychotropically potent as delta-9-THC. The same ratio of activity was observed on i.v. administration.
Delta-9-THC (4 mg/kg i.m.) blocked the emetic response in cats caused by cisplatin (7.5 mg/kg i.v.) [25]. The metabolite 11-hydroxy-delta-9-THC, which is considerably more psychotropic than delta-9-THC, was less antiemetic than delta-9-THC showing that, in cats at least, there is no parallelism between the psychotropic effects and the antiemetic ones. Indeed, we have recently shown that a non-psychotropic cannabinoid (HU-211) is more potent than delta-9-THC as an antiemetic [7].
The LD50 values for Fischer rats treated orally with single doses of delta-9-THC and delta-8THC, and observed for 7 days, are 1910 mg/kg and 1980 mg/kg (for males) respectively and 860 mg/kg (for females) [26]. The histopathological changes caused by these extremely high doses were essentially the same for both delta-8-and delta-9-THC. LD50 could not be determined in either rhesus monkeys or dogs as single oral doses of up to 9000 mg/kg of either delta-8- or delta-9-THC in dogs or monkeys were non-lethal. Histopathological alterations did not occur in either dogs or monkeys. A chronic oral toxicity study in rats with both isomers has been reported. delta-8-THC was found to be slightly less toxic than the delta-9 isomer [27]. With delta-8-THC, after 119 days of consecutive administration, no deaths were observed in males with daily doses of up to 400 mg/kg; 1/10 deaths occurred at 500 mg/kg. With females, no deaths were caused by doses of up to 250 mg/kg; 5/13 deaths were recorded at 400 mg/kg and 12/67 were recorded at 500 mg/kg. The above described animal and human data indicated that delta-8-THC can be safely administered to human patients.
We found, as expected, that young children with different hematologic cancers, who were treated with a variety of anticancer drug protocols, could be administered doses of delta-8-THC considerably higher than the doses of delta-9-THC generally administered to adult cancer patients without the occurrence of major side effects, (5-10 mg/m2 of delta-9-THC generally recommended for adult patients [28] versus 18 mg/m2 of delta-8-THC used by us in children). As mentioned above, the prevention of vomiting was complete, regardless of the antineoplastic protocol followed . We observed no delayed nausea or vomiting. Although the number of pediatric cancer patients treated so far is small, the total number of treatments is considerable (480 times) as most patients underwent several treatment cycles. Without the cannabinoid therapy we would have expected the patients to vomit in most treatments.
In summary, the complete success in preventing vomiting due to antineoplastic treatment in children, and the essential lack of side effects, leads us to believe that delta-8-THC at a dose considerably higher than the doses of delta-9-THC usually administered to adults, can serve as a new, inexpensive antiemetic agent in pediatric cancer chemotherapy.
Reprinted by permission of the publisher from Abrahamov, Aya. Avraham Abrahamov and Raphael Mechoulam 1995. An efficient new cannabinoid antiemetic in pediatric oncology. Life Sciences 56(23/24); 2097-2102. Copyright 1995 by Elsevier Science Inc.
References
- Mechoulam, R., 1986. In R. Mechoulam (ed.) Cannabinoids as Therapeutic Agents, CRC Press, Boca Raton, FL: 1-20.
- Gaoni, Y. and R. Mechoulam, 1964. J. Am. Chem. Soc. 86: 1646.
- Sallan, S. E. et. al., 1975. N. Engl. J. Med. 293: 795-97.
- Levitt, M., 1986. In Mechoulam R, (ed.) Cannabinoids as Therapeutic Agents, CRC Press, Boca Raton, FL: 71-84.
- Plasse, T. F. et. al., 1991. Pharmacol. Biochem. Behav. 40: 695-700.
- Razdan, R. K., 1986. Pharmacol. Revs. 38: 75-149.
- Feigenbalm, S. A. et. al., 1989. Eur J. Pharmacol. 169: 159-165.
- Markham, A. and E. M. Sorkin, 1933. Drugs 45: 931-952.
- Gaoni, Y. and R. Mechoulam, 1966. Tetrahedron 22: 1481-1488.
- Capizzi, R. L. et. al., 1985. Semin. Oncol. l2 (Suppl 3): 105-113.
- Connors, J. M. and P. Klimo, 1987. Semin. Hematol. 24 (Suppl. 1): 3540.
- Standard Israeli National Protocol based on BFM protocols, see for example Henze, G. et. al. 1982 Klin. Pediat. 19(1): 195-203.
- National Wilms Tumor Study-4. Stage III and IV/Favorable histology; Stage I-IV Oclear cell sarcoma. Provided by Dr. Daniel Green and the Roswell Park Memorial Institute.
- Arlin, S. A. et al., 1987. J. Clin. Oncol. 5: 371-375.
- Magrath, I. T. et. al., 1984. Blood 63: 1102-1111.
- Nimeyer, C. M. et. al. 1985 Semin. Oncol. L2: 122-130.
- Mechoulam, R., 1973. In Mechoulam, R. ed. Marihuana. Chemistry, Pharmacology, Metabolism and Clinical Effects, Academic Press, New York 1-99.
- Harvey, D. J. and W. D. M. Paton, 1984. Revs. Bioch. Toxic. 6: 221-264.
- Martin, B. R., 1986.. Pharmacol. Revs. 38: 45-74.
- Dewey, W. L., 1986. Pharmacol. Revs. 38: 151-178.
- Pertwee, R. G., 1988. Pharmac. Ther. 36: 189-261.
- Schekel, C. L. et. al., 1968. Science 160: 1467-1469.
- Grunfeld, Y. and H. Edery, 1969. Psychopharmacologia 24: 200-210.
- Hollister, L. E. and H. K. Gillespie, 1973 Clin. Pharmacol. Ther., 14: 353-357.
- McCarthy, L. E. et. al., 1984. In Agurell, S. Dewey DL, Willette RE, (eds) The Cannabinoids: Chemical, Pharmacologic and Therapeutic Aspects, Acad. Press, Orlando, FL: 859-870.
- Thompson, G. R. et. al. 1973. Toxicol. Appl. Pharmacol. 25: 363-372.
- Thompson, G. R. et. al., 1973. Toxicol. Appl. Pharmacol. 25: 373-390.
- Anonymous, 1985. Synthetic marijuana for nausea and vomiting due to cancer chemotherapy. Medical Lett. 27: 97-98.
“Medical marijuana ... in the hospital?”
As states legalize marijuana, hospitals develop policies on inpatient use
By Mollie Durkin
Hospitals have been going green, in the sense of sustainability, for a while, but recently the term has taken on a whole new meaning. With medical marijuana (aka cannabis) laws now in effect in more than half the country, hospitals are seeing more patients who have been certified to use the drug, and they are developing policies and practices in response.
Although marijuana remains illegal under federal law as a Schedule I drug, more states voted last November to give the green light to recreational (California, Maine, Massachusetts, and Nevada) and medical (Florida, North Dakota, and Arkansas) cannabis use, bringing the overall recreational count to eight states and the medical count to 28 states and Washington, D.C.
At the same time, surveys show Americans becoming more tolerant of and open to medical marijuana. About 75% believe medical marijuana should be legal in the U.S., and 33% would be likely to use it to treat pain if advised by a physician, according to a 2016 Prevention Magazine survey of 1,025 U.S. adults. A 2014 WebMD poll of 1,544 doctors also found support for medical marijuana, with 67% believing it should be a medical option for patients on a local level and 56% supporting nationwide legalization.
So even if your hospital isn't in a green state, it may be time to start considering what an inpatient medical marijuana policy would look like. Which patients are permitted to receive the substance, where should it be stored, who should administer it, and should it be documented in the EHR?
Opting in
In 2015, the Minnesota Hospital Association crafted some answers to those questions after the state legalized medical use. The association came up with three sample policies in line with three clear stances that hospitals can take on the issue, according to Rahul Koranne, MD, MBA, FACP, chief medical officer for the Minnesota Hospital Association (see sidebar).
“There was a very broad contingent of leaders—and I'm really proud of them—that said, ‘This particular substance is being shown to help some of our patients, especially the pediatric patients. Our mission is to serve our patients and their families, so we just cannot say broadly this will not be allowed within our walls,’ which is why these three policies materialized,” he said.
To create the policy templates, the association organized a medical cannabis committee and began a series of meetings, gaining continuous feedback from the state's health systems along the way, Dr. Koranne said. “It was very clear right off the bat that ... this particular workflow involves every department within the health system: the primary care clinics, specialty clinics, ED, ICU, medical units,” he said.
In addition to physicians, nurses, and pharmacists, representatives from external agencies (e.g., drug diversion, members of various professional boards) must be involved from the beginning in crafting such a policy, Dr. Koranne said, noting the importance of including legal counsel. The state's medical cannabis manufacturers were also involved. “We asked them to bring in the bottle, the product, and the label so our members and we could start becoming more familiar with what our patients and families will be bringing in,” he said.
At Mayo Clinic's hospitals in Rochester, Minn., medical cannabis use is permitted among patients registered with the state's program who come in with a product in its original container as dispensed by the state's approved cannabis patient centers, said Peter J. Post, PharmD, director of pharmacy quality and compliance. To date, more than 3,700 patients are actively enrolled in the program, according to the Minnesota Department of Health's Office of Medical Cannabis.
If such a patient is hospitalized, the admitting physician must decide whether continuation of the therapy is appropriate for the hospital stay, Dr. Post said. If the decision is made to continue the therapy, the physician would write an order for its continuation to communicate approved continued use during the hospital stay to the nursing and pharmacy staff, integrating that decision into the medication use process support systems, he said. Dr. Post also noted that only capsules and oral liquid are allowed, that the medication is not stored in or dispensed by the pharmacy, and that patients are not permitted to self-administer.
So far, medical cannabis use at Mayo's Minnesota hospitals isn't common. “Less than two patients per month on average to date. It wasn't the big crush that we thought it might've been,” Dr. Post said. He noted inpatient use has been most common in pediatric patients.
One factor that may have made it easier for Minnesota hospitals to open up to medical cannabis is that the state's standards for ensuring quality control are quite strong, and manufacturers are required to demonstrate consistency of product content, purity, stability, and accuracy of labeling, Dr. Post noted. “That's something that you don't see in many other states, in essence of that level of having some of the principles of medication quality control standards,” he said.
Opting out
In Maine, medical cannabis has been legal for years, but hospitals across the state commonly prohibit the use of the drug in their facilities.
Such policies are put to the test when patients intentionally or accidentally violate them. In 2015, a Maine registered medical marijuana patient, hospitalized for two weeks with a blood infection, tried to treat himself by rubbing an infused lotion onto his hands to relieve pain and stiffness from carpal tunnel. The hospital told the patient he needed to remove the substance from the hospital or it would be confiscated, the Portland Press Herald reported.
The hospital's prohibitive policy was related to concerns about losing its federal license, which does not allow for a Schedule I controlled substance to be on the premises, a hospital spokesman told the newspaper. These concerns are prevalent among other Maine hospitals, as well, said lobbyist Jeffrey A. Austin, vice president of governmental affairs and communications for the Maine Hospital Association in Augusta. “As long as CMS doesn't allow it and the FDA doesn't allow it to be prescribed, our members feel fairly confident that they need to continue to prohibit its use,” he said.
Although the risk of a hospital losing licensure or CMS certification for violating this regulation is small, the consequences could be enormous, Mr. Austin said. “When the state has considered this, we've always said, ‘OK, it is a remote risk, but who's bearing it? The hospital is. Would the state like to bear it and fully compensate the hospital for its loss of licensure?’... And nobody's ever taken me up on it,” he said.
Beyond legal concerns, hospital physicians contemplating medical marijuana use in their patients often have clinical worries, Mr. Austin said. “Most patients wouldn't just start taking something; they'd ask, ‘I'm sick, you've put me on all these IVs and drugs, can I keep taking my marijuana?’ A lot of clinicians wouldn't know how to answer that question because of the lack of research on cannabis, drug interactions, and so forth,” he said.
Mr. Austin noted that hospital administrators in the state aren't necessarily “dead set” against medical marijuana and that they'd like to see it go through the FDA process of rigorous review, which is stymied by its Schedule I status.
The only area where Maine hospitals have clear inconsistencies in medical marijuana policies is otherwise-untreatable pediatric epilepsy, he said. According to patient reports, “You'll find some hospitals that openly accept it, some that sort of shut the curtain and recognize that you may be doing it, and others that continue to say no,” Mr. Austin said.
Shifting rules
Clinicians do not prescribe or dispense medical marijuana; they recommend it in accordance with state law. Before making such a recommendation, they must typically certify a patient as having a state-approved qualifying medical condition (e.g., HIV/AIDS, inflammatory bowel disease).
Although the certification process typically occurs outside the hospital, states are including hospitals in related legislation. As of May 2016, state laws in Connecticut and Maine permit the use of medical marijuana by hospitalized patients and give some state-level legal protection for clinicians who administer it. “That's appreciated because certainly some hospitals are allowing some usage, particularly in the pediatric epilepsy world,” Mr. Austin said.
Such regulations may make clinicians and hospitals somewhat more comfortable allowing medical marijuana, but the federal prohibition is still a significant issue. “The feds, unquestionably, have to lead on this issue,” said Mr. Austin. Even if there isn't a statewide policy on how hospitals should act in the context of medical marijuana, individual hospitals should work to create policies and enact them across the institution, said Jeanette Marie Tetrault, MD, FACP, associate professor of medicine at the Yale School of Medicine in New Haven, Conn. “Hospitals should come up with...a multidisciplinary committee to really think these questions through because I think we're going to start seeing it more and more,” she said, listing addiction specialists, pain clinicians, and psychiatrists as important participants.
Dr. Tetrault pointed out that many states vote by referendum on which medical indications are able to be treated with medical marijuana. “This is not physicians sitting at the table, deciding what the indications are going to be.... We weren't allowed to be at the table when the laws were being made, so it'd be nice to be at the table when the hospitals are trying to make a policy about it,” she said.
As states legalize marijuana, hospitals develop policies on inpatient use
By Mollie Durkin
Hospitals have been going green, in the sense of sustainability, for a while, but recently the term has taken on a whole new meaning. With medical marijuana (aka cannabis) laws now in effect in more than half the country, hospitals are seeing more patients who have been certified to use the drug, and they are developing policies and practices in response.
Although marijuana remains illegal under federal law as a Schedule I drug, more states voted last November to give the green light to recreational (California, Maine, Massachusetts, and Nevada) and medical (Florida, North Dakota, and Arkansas) cannabis use, bringing the overall recreational count to eight states and the medical count to 28 states and Washington, D.C.
At the same time, surveys show Americans becoming more tolerant of and open to medical marijuana. About 75% believe medical marijuana should be legal in the U.S., and 33% would be likely to use it to treat pain if advised by a physician, according to a 2016 Prevention Magazine survey of 1,025 U.S. adults. A 2014 WebMD poll of 1,544 doctors also found support for medical marijuana, with 67% believing it should be a medical option for patients on a local level and 56% supporting nationwide legalization.
So even if your hospital isn't in a green state, it may be time to start considering what an inpatient medical marijuana policy would look like. Which patients are permitted to receive the substance, where should it be stored, who should administer it, and should it be documented in the EHR?
Opting in
In 2015, the Minnesota Hospital Association crafted some answers to those questions after the state legalized medical use. The association came up with three sample policies in line with three clear stances that hospitals can take on the issue, according to Rahul Koranne, MD, MBA, FACP, chief medical officer for the Minnesota Hospital Association (see sidebar).
“There was a very broad contingent of leaders—and I'm really proud of them—that said, ‘This particular substance is being shown to help some of our patients, especially the pediatric patients. Our mission is to serve our patients and their families, so we just cannot say broadly this will not be allowed within our walls,’ which is why these three policies materialized,” he said.
To create the policy templates, the association organized a medical cannabis committee and began a series of meetings, gaining continuous feedback from the state's health systems along the way, Dr. Koranne said. “It was very clear right off the bat that ... this particular workflow involves every department within the health system: the primary care clinics, specialty clinics, ED, ICU, medical units,” he said.
In addition to physicians, nurses, and pharmacists, representatives from external agencies (e.g., drug diversion, members of various professional boards) must be involved from the beginning in crafting such a policy, Dr. Koranne said, noting the importance of including legal counsel. The state's medical cannabis manufacturers were also involved. “We asked them to bring in the bottle, the product, and the label so our members and we could start becoming more familiar with what our patients and families will be bringing in,” he said.
At Mayo Clinic's hospitals in Rochester, Minn., medical cannabis use is permitted among patients registered with the state's program who come in with a product in its original container as dispensed by the state's approved cannabis patient centers, said Peter J. Post, PharmD, director of pharmacy quality and compliance. To date, more than 3,700 patients are actively enrolled in the program, according to the Minnesota Department of Health's Office of Medical Cannabis.
If such a patient is hospitalized, the admitting physician must decide whether continuation of the therapy is appropriate for the hospital stay, Dr. Post said. If the decision is made to continue the therapy, the physician would write an order for its continuation to communicate approved continued use during the hospital stay to the nursing and pharmacy staff, integrating that decision into the medication use process support systems, he said. Dr. Post also noted that only capsules and oral liquid are allowed, that the medication is not stored in or dispensed by the pharmacy, and that patients are not permitted to self-administer.
So far, medical cannabis use at Mayo's Minnesota hospitals isn't common. “Less than two patients per month on average to date. It wasn't the big crush that we thought it might've been,” Dr. Post said. He noted inpatient use has been most common in pediatric patients.
One factor that may have made it easier for Minnesota hospitals to open up to medical cannabis is that the state's standards for ensuring quality control are quite strong, and manufacturers are required to demonstrate consistency of product content, purity, stability, and accuracy of labeling, Dr. Post noted. “That's something that you don't see in many other states, in essence of that level of having some of the principles of medication quality control standards,” he said.
Opting out
In Maine, medical cannabis has been legal for years, but hospitals across the state commonly prohibit the use of the drug in their facilities.
Such policies are put to the test when patients intentionally or accidentally violate them. In 2015, a Maine registered medical marijuana patient, hospitalized for two weeks with a blood infection, tried to treat himself by rubbing an infused lotion onto his hands to relieve pain and stiffness from carpal tunnel. The hospital told the patient he needed to remove the substance from the hospital or it would be confiscated, the Portland Press Herald reported.
The hospital's prohibitive policy was related to concerns about losing its federal license, which does not allow for a Schedule I controlled substance to be on the premises, a hospital spokesman told the newspaper. These concerns are prevalent among other Maine hospitals, as well, said lobbyist Jeffrey A. Austin, vice president of governmental affairs and communications for the Maine Hospital Association in Augusta. “As long as CMS doesn't allow it and the FDA doesn't allow it to be prescribed, our members feel fairly confident that they need to continue to prohibit its use,” he said.
Although the risk of a hospital losing licensure or CMS certification for violating this regulation is small, the consequences could be enormous, Mr. Austin said. “When the state has considered this, we've always said, ‘OK, it is a remote risk, but who's bearing it? The hospital is. Would the state like to bear it and fully compensate the hospital for its loss of licensure?’... And nobody's ever taken me up on it,” he said.
Beyond legal concerns, hospital physicians contemplating medical marijuana use in their patients often have clinical worries, Mr. Austin said. “Most patients wouldn't just start taking something; they'd ask, ‘I'm sick, you've put me on all these IVs and drugs, can I keep taking my marijuana?’ A lot of clinicians wouldn't know how to answer that question because of the lack of research on cannabis, drug interactions, and so forth,” he said.
Mr. Austin noted that hospital administrators in the state aren't necessarily “dead set” against medical marijuana and that they'd like to see it go through the FDA process of rigorous review, which is stymied by its Schedule I status.
The only area where Maine hospitals have clear inconsistencies in medical marijuana policies is otherwise-untreatable pediatric epilepsy, he said. According to patient reports, “You'll find some hospitals that openly accept it, some that sort of shut the curtain and recognize that you may be doing it, and others that continue to say no,” Mr. Austin said.
Shifting rules
Clinicians do not prescribe or dispense medical marijuana; they recommend it in accordance with state law. Before making such a recommendation, they must typically certify a patient as having a state-approved qualifying medical condition (e.g., HIV/AIDS, inflammatory bowel disease).
Although the certification process typically occurs outside the hospital, states are including hospitals in related legislation. As of May 2016, state laws in Connecticut and Maine permit the use of medical marijuana by hospitalized patients and give some state-level legal protection for clinicians who administer it. “That's appreciated because certainly some hospitals are allowing some usage, particularly in the pediatric epilepsy world,” Mr. Austin said.
Such regulations may make clinicians and hospitals somewhat more comfortable allowing medical marijuana, but the federal prohibition is still a significant issue. “The feds, unquestionably, have to lead on this issue,” said Mr. Austin. Even if there isn't a statewide policy on how hospitals should act in the context of medical marijuana, individual hospitals should work to create policies and enact them across the institution, said Jeanette Marie Tetrault, MD, FACP, associate professor of medicine at the Yale School of Medicine in New Haven, Conn. “Hospitals should come up with...a multidisciplinary committee to really think these questions through because I think we're going to start seeing it more and more,” she said, listing addiction specialists, pain clinicians, and psychiatrists as important participants.
Dr. Tetrault pointed out that many states vote by referendum on which medical indications are able to be treated with medical marijuana. “This is not physicians sitting at the table, deciding what the indications are going to be.... We weren't allowed to be at the table when the laws were being made, so it'd be nice to be at the table when the hospitals are trying to make a policy about it,” she said.
Are We Missing Something?

During the Inaugural Institute of Cannabis Research (ICR) at Colorado State University-Pueblo, this international, multidisciplinary cannabis research conference set for April 28-30th 2017, on the Colorado State University-Pueblo campus. The keynote address on Saturday will be presented by none other than, “The Scientist”, Raphael Mechoulam, Ph.D., who is considered “the father of cannabis research.”
The ICR conference will celebrate a myriad of research and intellectual pursuits from internationally renowned speakers and pioneering cannabis scholars. The preliminary program provides information on more than 70 scheduled presentations from 100+ state, national, and international cannabis researchers from private research organizations, prominent universities, state and national government agencies, and industry representatives.
Dr. Mechoulam is a pioneer in the field of cannabis research and a discoverer of the endocannabinoid system. Dr. Mechoulam’s keynote address at the ICR conference is titled: The Endocannabinioid System: A Look Back and Ahead. Raphael Mechoulam, Ph.D., who is considered “the father of cannabis research,” will present the inaugural Mechoulam Lecture, which will commemorate the groundbreaking discoveries that have made contemporary cannabis science
possible. Dr. Mechoulam is professor in the Department of Medicinal Chemistry at the Institute of Drug Research at Hebrew University in Israel.
possible. Dr. Mechoulam is professor in the Department of Medicinal Chemistry at the Institute of Drug Research at Hebrew University in Israel.
Dr. Mechoulam is an Israeli organic chemist and professor of Medicinal Chemistry at the Hebrew University of Jerusalem in Israel. He was among the first to complete the total synthesis of the major plant cannabinoids Δ9-tetrahydrocannabinol, cannabidiol, cannabigerol, and others. Dr. Mechoulam also played a key role in the isolation of the first described endocannabinoid anandamide.
Prof. Mechoulam received his Masters Degree in Biochemistry from the Hebrew University in 1952 and his Ph.D. from the Weizmann Institute in 1958 where he studied under Professor F. Sondheimer. He completed his postdoctoral research at the Rockefeller Institute. Dr. Mechoulam is currently with the Institute for Drug Research at the Faculty of Medicine at the Hebrew University in Jerusalem. He is former Rector of the University and is a member of the Israel Academy of Sciences.
Dr. Mechoulam has received many honours, including honorary doctorates from Spain and USA, the Israel Prize in 2000 and the European College of Neuropsychopharmacology Lifetime Achievement Award in 2006. In 2012, he received the Rothschild Prize. His research interests are in the field of the chemistry and biological activity of natural products and medicinal agents. His main contributions are in the field of the constituents of cannabis and the endogenous cannabinoids found in the brain and the periphery. He has published extensively on their pharmacological activities.
Prof. Mechoulam received his Masters Degree in Biochemistry from the Hebrew University in 1952 and his Ph.D. from the Weizmann Institute in 1958 where he studied under Professor F. Sondheimer. He completed his postdoctoral research at the Rockefeller Institute. Dr. Mechoulam is currently with the Institute for Drug Research at the Faculty of Medicine at the Hebrew University in Jerusalem. He is former Rector of the University and is a member of the Israel Academy of Sciences.
Dr. Mechoulam has received many honours, including honorary doctorates from Spain and USA, the Israel Prize in 2000 and the European College of Neuropsychopharmacology Lifetime Achievement Award in 2006. In 2012, he received the Rothschild Prize. His research interests are in the field of the chemistry and biological activity of natural products and medicinal agents. His main contributions are in the field of the constituents of cannabis and the endogenous cannabinoids found in the brain and the periphery. He has published extensively on their pharmacological activities.
About The Documentary, “The Scientist”, His Life And Work
In 1964 Professor Raphael Mechoulam was on a public bus carrying 5 kilos of premium Lebanese hashish in a plastic bag to his laboratory at the Weitzmann Institute in Rehovot. That noticeably fragrant bus ride turned out to be a fateful one, as Mechoulam used his haul to discover the psychoactive component in Cannabis, Tetrahydrocannabinol (THC). It was a discovery that had eluded scientists for decades. Twenty years later, Mechoulam ascertained that THC interacts with the largest receptor system in the human body, the endocannabinoid system (ECS). He then found that the human brain produces its very own cannabis—a chemical that they named anandamide after the Sanskrit word ananda, “bliss.”
http://mechoulamthescientist.com/about-the-scientist/
Though still unknown to most researchers and medical professionals because of the worldwide prohibition of marijuana, the importance of the endocannabinoid system is growing daily. It has been called the “supercomputer that regulates homeostasis in the human body.” Because receptors are found throughout the brain and in every major organ, this system is thought to be involved in most disease state. This is one reason that cannabis treats so many different illnesses. Mechoulam has been investigating this compound longer and more thoughtfully than any other scientist. He has unearthed cannabis’s role in treating seizure disorders, schizophrenia and PTSD, as well as on other functions that govern human health like infant-maternal bonding. He has been awarded numerous scientific prizes and is universally acknowledged as the “father of cannabinoid medicine.” Despite these accolades, Mechoulam’s name isn’t known outside of a small group of researchers.
“The Scientist is a documentary that traces the story of Mechoulam from his early days as a child of the Holocaust in Bulgaria, through his immigration to Israel, and his career as the chief investigator into the chemistry and biology of the world’s most misunderstood plant.
“When Darwin finished his ideas on evolution he put them in a drawer for 20 years because he feared what the Church would say,” says Zach Klein, the writer, producer, editor of The Scientist. “Mechoulam was never vilified because he is such a great scientist, but the world has been slow to understand his findings because of the demonization that cannabis suffered since the beginning of the war on drugs.”
Klein first met Professor Mechoulam when researching the ways Cannabis reduces the symptoms of chemotherapy that his mother was experiencing while being treated for breast cancer. That led to his first documentary, Prescribed Grass, which aired on Israeli television in 2009 and prompted health officials in that country to launch what is today the world’s largest state-sponsored medical marijuana program. By EurpoaWire on July 31, 2015
- Somach Sachs Prize for “best research by a scientist below 35 at the Weizmann Institute”, 1964.
- Distinguished Visiting Professorship, Ohio State University, Columbus, Ohio, 1982-1983.
- “Pharmacology, Biochemistry and Behavior” Nov. 1991 issue dedicated to R.Mechoulam. for achievements in the cannabinoid field.
- Elected, Member Israel Academy of Sciences, 1994.
- David R. Bloom Prize, 1998, for “excellence in pharmaceutical research”, Hebrew University.
- The International Cannabinoid Research Society (ICRS) establishes an annual award to be named The R. Mechoulam Annual Award in Cannabinoid Research, 1999.
- Israel Prize in Exact Sciences – chemistry, 2000.
- Ariens Award and Lecture. 2000. Dutch Pharmacological Society sponsored by Solvay Pharmaceuticals. Amsterdam.
- Doctor Honoris Causa, Ohio State University, Columbus, Ohio, 2001.
- Elected, Honorary Member, Israel Society of Physiology and Pharmacology, 2002.
- Heinrich Wieland Prize, to promote research on “lipids and related substances in the fields of Chemistry, Biochemistry, Physiology, and Clinical Medicine”, Munich, Germany, 2004.
- Henrietta Szold Prize for achievements in medical research, Tel-Aviv Municipality, June 2005.
- Doctor Honoris Causa, Complutense University, Madrid, 2006. ECNP (European College of Neuropsychopharmaclogy), Lifetime Achievement Award, Paris, 2006.
- ICRS (International Cannabinoid Research Society) Special Award For lifetime achievements in the cannabinoid field, Cologne, Germany, 2007.
- Israel Chemical Society Prize for excellence in research, Feb. 2009.
- Hebrew University, Medical Faculty Prize for excellence in research, June 2010.
- Eicosanoid Research Foundation Lifetime Achievement Award, Seattle, Washington, September, 2011.
- NIDA Discovery Award, NIH, Bethesda, September 2011.
- Rothschild Prize by Keren Hanadiv (The Rothschild Family Foundation), Jerusalem (in the Knesset) 2012.
- EMET Prize – to be presented by the Prime Minister in November, 2012.
Rules, Regulations, & Policy Solution For The Petition: Requesting The Inclusion Of A New Medical Treatment: Pediatric Oncology And Cannabis Use for Antiemetic In State Hospitals
The approval of this Petition: Requesting The Inclusion Of A New Medical Treatment: Pediatric Oncology And Cannabis Use for Antiemetic In State Hospitals, that is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department to create Rules and Regulations for medical cannabis use in hospitals in New Mexico for Pediatric Oncology And Cannabis Use for Antiemetic as the Lynn and Erin Compassionate Use Act does allow for.
The approval of this petition would bring the Department of Health in compliance with the intent of the law and uphold the spirit of the Lynn and Erin Compassionate Use Act, 2007. Fulfilling both;“ Section 2. PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments” And Section 6. ADVISORY BOARD CREATED--DUTIES: The advisory board shall: A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis.” New Mexico’s medical cannabis history started in 1978. After public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis...the first law.
References (not listed above)
Understanding medical cannabis.Elemental Wellness Center, 2014 Jul.
Appendix A:
WHEREAS cannabis (marijuana) has been used as a medicine for at least 5,000 years and can be effective for serious medical conditions for which conventional medications fail to provide relief;
WHEREAS modern medical research has shown that cannabis can slow the progression of such serious diseases as Alzheimer’s and Parkinson’s and stop HIV and cancer cells from spreading; has both anti-inflammatory and pain-relieving properties; can alleviate the symptoms of epilepsy, PTSD and multiple sclerosis; is useful in the treatment of depression, anxiety and other mental disorders; and can help reverse neurological damage from brain injuries and stroke;
WHEREAS the World Health Organization has acknowledged the therapeutic effects of cannabinoids, the primary active compounds found in cannabis, including as an anti-depressant, appetite stimulant, anticonvulsant and anti-spasmodic, and identified cannabinoids as beneficial in the treatment of asthma, glaucoma, and nausea and vomiting related to illnesses such as cancer and AIDS;
WHEREAS the American Medical Association has called for the review of the classification of cannabis as a Schedule I controlled substance to allow for clinical research and the development of cannabinoid-based medicines;
WHEREAS the National Cancer Institute has concluded that cannabis has antiemetic effects and is beneficial for appetite stimulation, pain relief, and improved sleep among cancer patients;
WHEREAS the American Herbal Pharmacopoeia and the American Herbal Products Association have developed qualitative standards for the use of cannabis as a botanical medicine;
WHEREAS the U.S. Supreme Court has long noted that states may operate as “laboratories of democracy” in the development of innovative public policies;
WHEREAS twenty-eight states and the District of Columbia have enacted laws that allow for the medical use of cannabis;
WHEREAS seventeen additional states have enacted laws authorizing the medical use of therapeutic compounds extracted from the cannabis plant;
WHEREAS more than 17 years of state-level experimentation provides a guide for state and federal law and policy related to the medical use of cannabis;
WHEREAS accredited educational curricula concerning the medical use of cannabis have been established that meets Continuing Medical Education requirements for practicing physicians;
WHEREAS Congress has prohibited the federal Department of Justice from using funds to interfere with and prosecute those acting in compliance with their state medical cannabis laws, and the Department of Justice has issued guidance to U.S. Attorneys indicating that enforcement of the Controlled Substances Act is not a priority when individual patients and their care providers are in compliance with state law, and that federal prosecutors should defer to state and local enforcement so long as a viable state regulatory scheme is in place.
WHEREAS modern medical research has shown that cannabis can slow the progression of such serious diseases as Alzheimer’s and Parkinson’s and stop HIV and cancer cells from spreading; has both anti-inflammatory and pain-relieving properties; can alleviate the symptoms of epilepsy, PTSD and multiple sclerosis; is useful in the treatment of depression, anxiety and other mental disorders; and can help reverse neurological damage from brain injuries and stroke;
WHEREAS the World Health Organization has acknowledged the therapeutic effects of cannabinoids, the primary active compounds found in cannabis, including as an anti-depressant, appetite stimulant, anticonvulsant and anti-spasmodic, and identified cannabinoids as beneficial in the treatment of asthma, glaucoma, and nausea and vomiting related to illnesses such as cancer and AIDS;
WHEREAS the American Medical Association has called for the review of the classification of cannabis as a Schedule I controlled substance to allow for clinical research and the development of cannabinoid-based medicines;
WHEREAS the National Cancer Institute has concluded that cannabis has antiemetic effects and is beneficial for appetite stimulation, pain relief, and improved sleep among cancer patients;
WHEREAS the American Herbal Pharmacopoeia and the American Herbal Products Association have developed qualitative standards for the use of cannabis as a botanical medicine;
WHEREAS the U.S. Supreme Court has long noted that states may operate as “laboratories of democracy” in the development of innovative public policies;
WHEREAS twenty-eight states and the District of Columbia have enacted laws that allow for the medical use of cannabis;
WHEREAS seventeen additional states have enacted laws authorizing the medical use of therapeutic compounds extracted from the cannabis plant;
WHEREAS more than 17 years of state-level experimentation provides a guide for state and federal law and policy related to the medical use of cannabis;
WHEREAS accredited educational curricula concerning the medical use of cannabis have been established that meets Continuing Medical Education requirements for practicing physicians;
WHEREAS Congress has prohibited the federal Department of Justice from using funds to interfere with and prosecute those acting in compliance with their state medical cannabis laws, and the Department of Justice has issued guidance to U.S. Attorneys indicating that enforcement of the Controlled Substances Act is not a priority when individual patients and their care providers are in compliance with state law, and that federal prosecutors should defer to state and local enforcement so long as a viable state regulatory scheme is in place.
No comments:
Post a Comment