
**Statement quoted from Governor Martinez (Highlighted) explains how ALL these Petitions for the Nov 2017 MCAB are ALL under authority of MCAB per the LECUA, 2007. **
New Mexico’s Medical Cannabis Program Expansion Is Now “Medically Necessary”
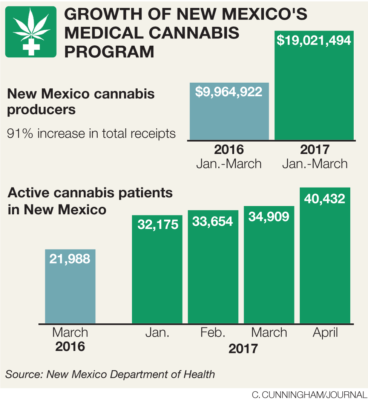
Today the New Mexico medical cannabis program has over 45,000 registered participants with 35 licensed (non-profit) producers growing 14,550 medical cannabis plants, as the program hits the midpoint of its 10th year. The Medical Cannabis Program (MCP) was created in 2007, as the Lynn and Erin Compassionate Use Act, under chapter 210 Senate Bill 523. The purpose of this Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
The State’s Medical Cannabis Program expansion is now “Medically Necessary”; the State needs to allow the Department of Health to open the application process to add more licensed non-profit producers, in conjunction with other measures to ensure safe access to medicine.
New Mexico’s medical cannabis history started in 1978. Lynn Pierson, a 26 year old cancer patient, brought the value of medical cannabis to the New Mexico legislature. After public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis. Later renamed The Lynn Pierson Marijuana & Research Act set forth a program that had over 250 New Mexicans receiving medical cannabis through the University of New Mexico until 1986. Federal opposition and state bureaucratic opposition developed thus ending the program in 1986.
Then in the early 2000’s, Erin Armstrong, a medical cannabis advocate who suffered from thyroid cancer, began to lobby the state legislature to pass a medical cannabis law. Armstrong, a Santa Fe High and UNM grad, spent three years tirelessly advocating for the medical cannabis program we have today. The Lynn and Erin Compassionate Use Act, 2007, passed under Governor Bill Richardson.
“Medically Necessary” is defined as “health-care services or supplies needed to prevent, diagnose, or treat an illness, injury, condition, disease, or its symptoms and that meet accepted standards of medicine.” Medical necessity is a United States legal doctrine, related to activities which may be justified as reasonable, necessary, and/or appropriate, based on evidence-based clinical standards of care.
Is the State out of Compliance with the MCP law, LECUA 2007? Yes.
For August 2017, there are 14,550 medical cannabis plants being grown for 45,000 registered program participants and that Equals 0.32 Medical Cannabis Plants per Patient. This is alarming as it is less than one plant per person and only a third of a fully grown/harvested medical cannabis plant is usable plant material for medicine. In 2016 there was 13,800 medical cannabis plants being grown for 32,175 registered program participants that Equaled 0.42 Medical Cannabis Plants per Patient. In 2015 there was 9,350 medical cannabis plants being grown for 12,647 registered program participants that Equaled 0.73 Medical Cannabis Plants per Patient. This is a program issue that has gone on for multiple years now and continues to get worse. Creating a serious health concern for registered program participants in addition to the serious liable aspects the State of New Mexico is also in.
The standards of care has been breached by the State of New Mexico with in the Medical Cannabis Program law; the purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
A standard of care is a medical or psychological treatment guideline, and can be general or specific. It specifies appropriate treatment based on scientific evidence and collaboration between medical and/or psychological professionals involved in the treatment of a given condition.
- 1 Licensed Non Profit Producer Per 1,300 Patient
- 35 LNPPs and 4 of those LNPPs have no operating dispensary;
additionally 4 LNPP's decided not to increase the number of plants they can grow;
of those four - 2 of these Licenses are being used to produce only 450 plants
- Average Price Per Gram (Flowers and Bud): $10.40
- Average Amount (Units) Purchased: 15.63
- (Average Transaction Amount: $162.55)
- Over Half of all Dispensary Locations are in Albuquerque City Area
- Totals Plants in Production: 12,281 (out of 13,800 possible)
- Number of Plants Harvested: 5,430
- 2017/2018 Relicensure; Total Medical Cannabis Plants = 14,550 (For over 45,000 Patients)
- If all 35 LNPPs grew the max allowed: (450 Medical Cannabis Plants x 35) Total = 15,750
“Pure mathematics is, in its way, the poetry of logical ideas.” ... Albert Einstein.
We have a sound law in the Lynn and Erin Compassionate Use Act that is benefiting many New Mexicans, yet we are unable to provide “adequate supply” and it can not be properly defined by the Department by using unknown variables it has not collected then this leads to further examination of how these definitions pertaining to adequate supply were determined in the past years. Let’s continue to allow the medical cannabis program to benefit and save lives of more and more New Mexicans.
The current plant count set at 450 plants allowed by each medical cannabis producers clearly cannot meet the demands of over 45,000 patients in the program. Complicating the matter further, not all the medical cannabis producers in the program are growing the allotted 450 plants. If all LNPPs were growing the 450 plants then there would be 15,750 plants available. New Mexico’s medical cannabis program saw a 75% increase in participants over the last year. The 2016/17 licensure list for the medical cannabis program shows a total of 13,800 medical cannabis plants licensed by the 35 producers for All registered program participants in the program.
For those rules and regulations that have been established limiting patients and primary caregivers to; “Pursuant to Department rule, a personal production license holder may possess no more than four (4) mature cannabis plants (flowering) and twelve (12) immature plants (non-flowering and male plants). A qualified patient may also possess no more than 230 units of usable cannabis within a three-month period. A unit is defined as one gram of dried usable cannabis plant material, or 0.2 grams (200 milligrams) of THC in a cannabis-derived product.”. This current format being used by the Department of Health Medical Cannabis Program in devising adequate supply does not allow for the beneficial use of medical cannabis. This in fact prevents patients from fully being able to alleviate symptoms caused by debilitating medical conditions and their medical treatments and that creates a liable situation for the state being out of compliance with the LECUA, 2007.
How Is The Medical Cannabis Program Out Of Compliance With The LECUA, 2007?
For example, a cancer patient in the medical cannabis program, to be able to receive beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments under the current law; cancer patients would need to be allowed to posses a minimum quantity of usable medical cannabis of 425.243 grams per 3 months (or 2.5 ounces every two weeks). For this patient scenario, in the patient having a PPL - the addition of two more medical cannabis plants or Patient / Caregiver safe access to medical cannabis via LPPC, would allow for this treatment. (Patient / Caregiver PPL plant count increased to allow for 6 immature seedlings /clones / cuttings, 6 plants in vegetative stage, and 6 plants in flowering stage for total of 18 cannabis plants. )
Types of medicine made from the medical cannabis plants for treating cancer is a concentrated medical cannabis oil. A three month supply of this concentrated medical cannabis oil requires 450-500 grams (or Units) of dried cannabis flower plant material. (The oil is also known as, hemp oil, Phoenix Tears, and Rick Simpson Oil (RSO), whole-plant cannabis oil can be orally administered or applied directly to the skin. Sublingual delivery is the preferred method of treatment for many cancer patients.)
A 30 day supply of cannabis oil is 60 grams or ml of oil with a dose of 2 grams or ml per day. It requires 450-500 grams of dried cannabis flower plant material to make high quality cannabis oil. So a 90 day supply or three months is 180 grams or ml of oil or 1425 grams of dried cannabis flower plant material ( Source: Rick Simpson ). Those rules and regulations that have been established limiting patients and primary caregivers to having only 16 medical cannabis plants with only 4 in flower for a PPL, and the limit to 230 Units (grams) of any amount of medical cannabis for a three month period does not allow for the beneficial use of medical cannabis and further prevents the purpose of the law to be fulfilled as stated in section two. This also does not allow for the beneficial use of medical cannabis for other medical cannabis medicine products like tinctures and medibles, which further prevents the purpose of the law to be fulfilled.
Those rules and regulations that have been established and the current plant count format & other petitions that are addressing … those rules and regs being used by the Department of Health Medical Cannabis Program in devising adequate supply does not allow for the beneficial use of medical cannabis. This in fact prevents every patient in the MCP from fully being able to alleviate symptoms caused by all of the qualifying debilitating medical conditions and their medical treatments and creates a liable situation for the state being out of compliance with the LECUA, 2007. Even if the patient or primary caregiver is granted the “Medical Exception” and provided the additional 115 Units (or grams) for a total of 345 Units (or grams), the state and MCP would still not be in compliance with the LECUA law.
Those rules and regulations that have been established limiting patients and primary caregivers to having only 16 medical cannabis plants with only 4 in flower for a PPL, and the limit to 230 Units (grams) of any amount of medical cannabis for a three month period; and this current format being used by the Department of Health Medical Cannabis Program in devising adequate supply does not allow for the beneficial use of medical cannabis. This in fact prevents every patient in the MCP from fully being able to alleviate symptoms caused by all of the qualifying debilitating medical conditions and their medical treatments and creates a liable situation for the state being out of compliance with the LECUA, 2007. Even if the patient or primary caregiver is granted the “Medical Exception” and provided the additional 115 Units (or grams) for a total of 345 Units (or grams), the state and MCP would still not be in compliance with the LECUA law.

Removing CBD strains from medical cannabis plants counts in New Mexico and other state programs for patients, caregivers and medical cannabis producers allowable plant count just makes sense. A revision to allow for 450 THC plants and 450 CBD Strains with a 1:1 - CBD:THC ratio (allowing CBD ratio to go above one but keeping THC at 1 or less in the ratio of potency). A patent was already awarded to part of the federal government, the U.S. Health and Human Services in 2003 (US6630507) that covers the use of CBD as a treatment for various neurodegenerative and inflammatory disorders.
In order for the Department of Health Medical Cannabis Program to allow for the medical treatment of cannabis, the Department must properly have “adequate supply”. For the Department to have “adequate supply” they would need to know the different amounts of plant material that goes into all the different types of medicine being produced in the MCP. Dried cannabis flower (bud), pre-rolls, edibles, tinctures, topicals/salves, and concentrated forms of cannabis- all require different amounts of cannabis plant material to produce. This is empirical data that has not been collected, studied or researched within the state’s medical cannabis program by the Department of Health.
In order for the Department of Health Medical Cannabis Program to allow for the medical treatment of cannabis, the Department must properly have “adequate supply”. For the Department to have “adequate supply” they would need to know the different amounts of plant material that goes into all the different types of medicine being produced in the MCP. Dried cannabis flower (bud), pre-rolls, edibles, tinctures, topicals/salves, and concentrated forms of cannabis- all require different amounts of cannabis plant material to produce. This is empirical data that has not been collected, studied or researched within the state’s medical cannabis program by the Department of Health.
Representatives Deborah A. Armstrong and Bill McCamley sponsored a Medical Cannabis Research bill, HB 155 in the 2017 Regular Legislative session. A research assessment of physical and pharmacokinetic relationships in cannabis production and consumption in New Mexico hasn't ever been done in relation to Equivalency in Portion and Dosage for the medical cannabis program. HB-155 passed this year in the House of Representatives (Y:41 N:26), only to be left in the Senate Judiciary Committee with no action taken on it when the lawmakers had the time to do so.
Representative Armstrong had also tried getting a medical cannabis research bill passed in 2015. The legislation in 2015 even had six additional legislative sponsors, passed two committees and then was intentionally left to die. This is empirical data that has not been collected within the state’s medical cannabis program by the Department of Health. Therefore “adequate supply” can not be properly defined by the department by using unknown variables it has not collected. This further prevents the Department of Health from being able to set a proper plant count for each kind of licensed producer in the program for the means of achieving adequate supply within the medical cannabis program as required by law.
Yet we often hear State Government and Lawmakers in New Mexico say how they need to learn more about medical cannabis or that there isn’t enough research for this or that; all the while the Roundhouse has now stopped medical cannabis research twice since 2015. And a patient petition to create program research was not even publically heard by the Medical Cannabis Advisory Board.
During the 2017 Regular Legislative Session, state lawmakers made efforts to legislate a number of changes to the state’s Medical Cannabis Program with over 25 different pieces of legislation, one of the bills vetoed by Gov. Susana Martinez, was House Bill-527, on Friday-April 7th 2017 (same day as the medical cannabis advisory board meeting), saying she did so in part because she didn’t want to “eliminate an important responsibility” of the Medical Cannabis Advisory Board. Health Secretary Lynn Gallagher, who has the final word on changes to the state Medical Cannabis Program, hasn’t decided whether to accept new conditions and petitions the board recommended yet.
That same Friday morning, on April 7th 2017, the Department of Health’s Medical Cannabis Advisory Board held a meeting exercising that important responsibility the Governor spoke of, that resulted in some of the following: The Medical Cannabis Advisory Board voted in favor of the following Petitions and recommended to add them into the program;
The addition of Patient Run Collectives would help relieve the medical cannabis plant count shortage.
•2017-005 Change/increase possession limit to 16 oz- Recommended to add to MCP 4-0
•2017-009 Removal of Max THC Content- Recommended Removal of Cap 4-0
•2017-005 Change/increase possession limit to 16 oz- Recommended to add to MCP 4-0
•2017-009 Removal of Max THC Content- Recommended Removal of Cap 4-0
Per the Department of Health’s legal counsel’s input, the following petitions numbered 3 and 11 were said that they would require statutory changes or are not covered under the duties of the MCAB and were not discussed at the MCAB meeting. Yet on that same day of this Medical Cannabis Advisory Board Meeting, the Governor of New Mexico said she didn’t want to take away this important responsibility of the MCAB...so according to the Governor these Petitions should have been heard?
The addition of this Petition would allow the MCAB to better exercise that important responsibility the Governor spoke of thru increased membership, thus leading to relieving the medical cannabis plant count shortage.
•2017-011 Add definition of Medical Treatment definition to LECUA and add Adequate
Supply
•2017-011 Add definition of Medical Treatment definition to LECUA and add Adequate
Supply
Petitions 8,10 and 23 concern the licensed producers and would require statutory changes and are not covered under the duties of the MCAB and will not be discussed. Once again, on that same day of this Medical Cannabis Advisory Board Meeting, the Governor of New Mexico said she didn’t want to take away this important responsibility of the MCAB...so according to the Governor these Petitions should have been heard?
Why was there a denial of hearing these petitions that are the “important responsibility” of the Medical Cannabis Advisory Board?
All of these petitions provide a solution to the State’s current violation to the LECUA law and items proposed in all of these petitions were also proposed and passed in one or both chambers of the State’s legislature with some dying in committee or being vetoed.
The inclusion of this petition would help relieve the medical cannabis plant count shortage.
•2017-010 Increase plants for licensed producers
•2017-010 Increase plants for licensed producers
The inclusion of this petition would help relieve the medical cannabis plant count shortage.
•2017-023 Develop MCP education and research components
•2017-023 Develop MCP education and research components
The inclusion of this petition would help relieve the medical cannabis plant count shortage.
The current law for the Medical Cannabis Program, passed in 2007, states the following, (Page 1/Section 2) “PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.”

A Policy Solution For The Adequate Supply of Medical Cannabis Plants.
The Governor’s Office has highlighted the importance of such priorities like; Ensuring Transparency and Ethics in Government, and Keeping all New Mexicans Safe. In the Roundhouse, one of the state legislators’ primary functions is to represent the people who elect them, but it is by no means their only function. They help to solve the numerous problems of their constituents, they serve on interim committees and they continually study new ideas for legislation. The Department of Health’s mission is to promote health and wellness, improve health outcomes, and assure safety net services for all people in New Mexico. And the purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
The State’s Medical Cannabis Program expansion is now “Medically Necessary”; the State needs to allow the Department of Health to open the application process to add more licensed non-profit producers, in conjunction with the addition of patient run collectives and allowing some producers to increase the plants they can grow. The State can allow the Department and Medical Cannabis Advisory Board to exercise that important responsibility they have to all New Mexicans, by opening up and accepting producer applications under newly created rules that would have 3 different licensing options.
The Medical Cannabis Program officials can create 3 different licensing options to include:
- A Licensed Producer to operate only as a grow facility for distribution to dispensaries.
- A Licensed Producer to operate only as a dispensary for distribution to patients.
- A LNPP to operate both as a grow facility and licensed for to operate dispensaries - with a limit of 3 store fronts per this type of license.
- In addition to reducing current and new licensing fee’s.
The approval of ALL the recommendations made by the Doctors on the Medical Cannabis Advisory Board, having the Department of Health to open the application process to add more licensed non-profit producers, and increasing the amount of medical cannabis plants a LNPPs and Patients can grow; would all need to be done to bring the State of New Mexico in compliance with the legal intent of the LECUA law and uphold the spirit of the Lynn and Erin Compassionate Use Act, 2007. As we have already saw these same recommendations supported by voters and lawmakers in the state’s legislature. New Mexico’s medical cannabis history started in 1978. After public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis...the first law.
Appendix A:
Americans For Safe Access is proud to announce the 2017 edition of their Medical Cannabis Access in the United States report. Beginning in 2014 ASA recognized the need to evaluate and compare the myriad of medical cannabis laws across the country. To this end they’ve worked with their members and patients nationwide to develop a grading matrix that would indicate how well a state's laws met the needs of patients.
With medical cannabis programs now encompassing 44 states, the District of Columbia and the territories of Puerto Rico and Guam, 300 million Americans (85% of the population) now live in states with medical cannabis laws.
This report is intended to help lawmakers and regulators learn from the successes and challenges faced by their peers in other states and get an objective evaluation of their own program.
With medical cannabis programs now encompassing 44 states, the District of Columbia and the territories of Puerto Rico and Guam, 300 million Americans (85% of the population) now live in states with medical cannabis laws.
This report is intended to help lawmakers and regulators learn from the successes and challenges faced by their peers in other states and get an objective evaluation of their own program.
(Click Image to view report.)
7.34.2.8 ADVISORY BOARD MEMBERSHIP REQUIREMENTS AND RESPONSIBILITIES:
A. Advisory board membership: The advisory board shall consist of eight practitioners representing the fields of neurology, pain management, medical oncology, psychiatry, infectious disease, family medicine and gynecology. The practitioners shall be nationally board-certified in their area of specialty and knowledgeable about the medical use of cannabis. The members shall be chosen for appointment by the secretary from a list proposed by the New Mexico medical society.
B. Duties and responsibilities: The advisory board shall convene at least twice per year to:
(1) review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis;
(2) recommend quantities of cannabis that are necessary to constitute an adequate supply for qualified patients and primary caregivers;
(3) accept and review petitions to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis and all lawful privileges under the act and implementing rules;
(4) issue recommendations concerning rules to be promulgated for the issuance of registry identification cards; and
(5) review conditions previously reviewed by the board and approved by the secretary for the purpose of determining whether to recommend the revision of eligibility criteria for persons applying under those conditions or to review new medical and scientific evidence pertaining to currently approved conditions.
C. Advisory board membership term: Each member of the advisory board shall serve a term of two years from the date of appointment by the secretary. No member may be removed prior to the expiration of his or her term without a showing of good cause by the secretary.
D. Chairperson elect: The advisory board shall elect by majority vote cast of the eight member board a chairperson and an alternate. The chairperson or alternate shall exercise all powers and duties prescribed or delegated under the act or this rule.
(1) Public hearing responsibilities: The chairperson shall conduct a fair and impartial proceeding, assure that the facts are fully elicited and avoid delay. The chairperson shall have authority to take all measures necessary for the maintenance of order and for the efficient, fair and impartial resolution of issues arising during the public hearing proceedings or in any public meeting in which a quorum of the advisory board are present.
(2) Delegation of chair: The chairperson may delegate their responsibility to an alternate. The alternate shall exercise all powers and duties prescribed or delegated under the act or this part.
E. Per diem and mileage: All advisory board members appointed under the authority of the act or this part will receive as their sole remuneration for services as a member those amounts authorized under the Per Diem and Mileage Act, Sections 10-8-1 et seq., NMSA 1978.
[7.34.2.8 NMAC - Rp, 7.34.2.8 NMAC, 2/27/2015]
A. Advisory board membership: The advisory board shall consist of eight practitioners representing the fields of neurology, pain management, medical oncology, psychiatry, infectious disease, family medicine and gynecology. The practitioners shall be nationally board-certified in their area of specialty and knowledgeable about the medical use of cannabis. The members shall be chosen for appointment by the secretary from a list proposed by the New Mexico medical society.
B. Duties and responsibilities: The advisory board shall convene at least twice per year to:
(1) review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis;
(2) recommend quantities of cannabis that are necessary to constitute an adequate supply for qualified patients and primary caregivers;
(3) accept and review petitions to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis and all lawful privileges under the act and implementing rules;
(4) issue recommendations concerning rules to be promulgated for the issuance of registry identification cards; and
(5) review conditions previously reviewed by the board and approved by the secretary for the purpose of determining whether to recommend the revision of eligibility criteria for persons applying under those conditions or to review new medical and scientific evidence pertaining to currently approved conditions.
C. Advisory board membership term: Each member of the advisory board shall serve a term of two years from the date of appointment by the secretary. No member may be removed prior to the expiration of his or her term without a showing of good cause by the secretary.
D. Chairperson elect: The advisory board shall elect by majority vote cast of the eight member board a chairperson and an alternate. The chairperson or alternate shall exercise all powers and duties prescribed or delegated under the act or this rule.
(1) Public hearing responsibilities: The chairperson shall conduct a fair and impartial proceeding, assure that the facts are fully elicited and avoid delay. The chairperson shall have authority to take all measures necessary for the maintenance of order and for the efficient, fair and impartial resolution of issues arising during the public hearing proceedings or in any public meeting in which a quorum of the advisory board are present.
(2) Delegation of chair: The chairperson may delegate their responsibility to an alternate. The alternate shall exercise all powers and duties prescribed or delegated under the act or this part.
E. Per diem and mileage: All advisory board members appointed under the authority of the act or this part will receive as their sole remuneration for services as a member those amounts authorized under the Per Diem and Mileage Act, Sections 10-8-1 et seq., NMSA 1978.
[7.34.2.8 NMAC - Rp, 7.34.2.8 NMAC, 2/27/2015]
7.34.2.10 ADVISORY BOARD PUBLIC HEARING PROCEDURES:
A. Public hearing requirement: The advisory board shall convene by public hearing at least twice per year to accept and review petitions requesting the inclusion of medical conditions, medical treatments or diseases to the list of debilitating medical conditions. Any meeting consisting of a quorum of the advisory board members held for the purpose of evaluating, discussing or otherwise formulating specific opinions concerning the recommendation of a petition filed pursuant to this rule, shall be declared a public hearing open to the public at all times, unless a portion of the hearing is closed to protect information made confidential by applicable state or federal laws. A petitioner or his or her representative may request to close a portion of the hearing to protect the disclosure of confidential information by submitting their request in writing and having that request delivered to medical cannabis program staff at least 48 hours prior to the hearing.
B. Location of the public hearing: Unless otherwise ordered by the advisory board, the public hearing shall be in held in New Mexico at a location sufficient to accommodate the anticipated audience.
C. Public hearing notice: The medical cannabis program manager or designee shall, upon direction from the advisory board chairperson, prepare a notice of public hearing setting forth the date, time and location of the hearing, a brief description of the petitions received, and information on the requirements for public comment or statement of intent to present technical evidence, and no later than 30 days prior to the hearing date, send copies, with requests for publication, to at least one newspaper of general circulation. The program manager or designee may further issue notice of the hearing by any other means the department determines to be acceptable to provide notice to the public.
D. Public hearing agenda: The department shall make available an agenda containing a list of specific items to be discussed or information on how the public may obtain a copy of such agenda.
E. Postponement of hearing: Request for postponement of a public hearing will be granted, by the advisory board for good cause shown.
F. Statement of intent to present technical evidence: Any individual or association of individuals who wish to present technical evidence at the hearing shall, no later than 15 days prior to the date of the hearing, file a statement of intent. The statement of intent to present technical evidence shall include:
(1) the name of the person filing the statement;
(2) indication of whether the person filing the statement supports or opposes the petition at issue;
(3) the name of each witness;
(4) an estimate of the length of the direct testimony of each witness;
(5) a list of exhibits, if any, to be offered into evidence at the hearing; and
(6) a summary or outline of the anticipated direct testimony of each witness.
G. Ex parte discussions: At no time after the initiation and before the conclusion of the petition process under this part, shall the department, or any other party, interested participant or their representatives discuss ex parte the merits of the petitions with any advisory board member.
H. Public hearing process: The advisory board chairperson shall conduct the public hearing so as to provide a reasonable opportunity for all interested persons to be heard without making the hearing unreasonably lengthy or cumbersome or burdening the record with unnecessary repetition.
(1) A quorum of the advisory board shall consist of three voting members.
(2) The advisory board chairperson or alternate shall convene each public hearing by:
(a) introduction of the advisory board members;
(b) statutory authority of the board;
(c) statement of the public hearing agenda; and
(d) recognition of the petitioner.
(3) Petitioner comment period. The petitioner or by representative may present evidence to the advisory board. The advisory board shall only consider findings of fact or scientific conclusions of medical evidence presented by the petitioner or by representative to the advisory board prior to or contemporaneously with the public hearing.
(4) Public comment period: The advisory board may provide for a public comment period. Public comment may be by written comment, verbal or both.
(a) Written comment: Any individual or association of individuals may submit written comment to the advisory board either in opposition or support of the inclusion of a medical conditions, medical treatments or diseases to the existing list of debilitating medical conditions contained under the act. All written comment shall adhere to the requirements of Subsection F of this section.
(b) Public comment: Any member of the general public may testify at the public hearing. No prior notification is required to present general non-technical statements in support of or in opposition to the petition. Any such member may also offer exhibits in connection with his testimony, so long as the exhibit is non-technical in nature and not unduly repetitious of the testimony.
I. Recording the hearing: Unless the advisory board orders otherwise, the hearing will be audio recorded. Any person, other than the advisory board, desiring a copy of the audio tapes must arrange copying with the medical cannabis program or designee at their own expense.
[7.34.2.10 NMAC - Rp, 7.34.2.10 NMAC, 2/27/2015]
7.34.2.11 ADVISORY BOARD RECOMMENDATION TO THE DEPARTMENT:
A. Advisory board recommendation: Upon final determination the advisory board shall provide to the secretary a written report of finding, which recommends either the approval or denial of the petitioner’s request. The written report of findings shall include a medical justification for the recommendation based upon the individual or collective expertise of the advisory board membership. The medical justification shall delineate between the findings of fact made by the advisory board and scientific conclusions of credible medical evidence.
B. Department final determination: The department shall notify the petitioner within 10 days of the secretary’s determination. A denial by the secretary regarding the inclusion of a medical conditions, medical treatments or diseases to the existing list of debilitating medical conditions contained under the act shall not represent a permanent denial by the department. Any individual or association of individuals may upon good cause re-petition the advisory board. All requests shall present new supporting findings of fact, or scientific conclusions of credible medical evidence not previously examined by the advisory board.
[7.34.2.11 NMAC - Rp, 7.34.2.11 NMAC, 2/27/2015]
A. Public hearing requirement: The advisory board shall convene by public hearing at least twice per year to accept and review petitions requesting the inclusion of medical conditions, medical treatments or diseases to the list of debilitating medical conditions. Any meeting consisting of a quorum of the advisory board members held for the purpose of evaluating, discussing or otherwise formulating specific opinions concerning the recommendation of a petition filed pursuant to this rule, shall be declared a public hearing open to the public at all times, unless a portion of the hearing is closed to protect information made confidential by applicable state or federal laws. A petitioner or his or her representative may request to close a portion of the hearing to protect the disclosure of confidential information by submitting their request in writing and having that request delivered to medical cannabis program staff at least 48 hours prior to the hearing.
B. Location of the public hearing: Unless otherwise ordered by the advisory board, the public hearing shall be in held in New Mexico at a location sufficient to accommodate the anticipated audience.
C. Public hearing notice: The medical cannabis program manager or designee shall, upon direction from the advisory board chairperson, prepare a notice of public hearing setting forth the date, time and location of the hearing, a brief description of the petitions received, and information on the requirements for public comment or statement of intent to present technical evidence, and no later than 30 days prior to the hearing date, send copies, with requests for publication, to at least one newspaper of general circulation. The program manager or designee may further issue notice of the hearing by any other means the department determines to be acceptable to provide notice to the public.
D. Public hearing agenda: The department shall make available an agenda containing a list of specific items to be discussed or information on how the public may obtain a copy of such agenda.
E. Postponement of hearing: Request for postponement of a public hearing will be granted, by the advisory board for good cause shown.
F. Statement of intent to present technical evidence: Any individual or association of individuals who wish to present technical evidence at the hearing shall, no later than 15 days prior to the date of the hearing, file a statement of intent. The statement of intent to present technical evidence shall include:
(1) the name of the person filing the statement;
(2) indication of whether the person filing the statement supports or opposes the petition at issue;
(3) the name of each witness;
(4) an estimate of the length of the direct testimony of each witness;
(5) a list of exhibits, if any, to be offered into evidence at the hearing; and
(6) a summary or outline of the anticipated direct testimony of each witness.
G. Ex parte discussions: At no time after the initiation and before the conclusion of the petition process under this part, shall the department, or any other party, interested participant or their representatives discuss ex parte the merits of the petitions with any advisory board member.
H. Public hearing process: The advisory board chairperson shall conduct the public hearing so as to provide a reasonable opportunity for all interested persons to be heard without making the hearing unreasonably lengthy or cumbersome or burdening the record with unnecessary repetition.
(1) A quorum of the advisory board shall consist of three voting members.
(2) The advisory board chairperson or alternate shall convene each public hearing by:
(a) introduction of the advisory board members;
(b) statutory authority of the board;
(c) statement of the public hearing agenda; and
(d) recognition of the petitioner.
(3) Petitioner comment period. The petitioner or by representative may present evidence to the advisory board. The advisory board shall only consider findings of fact or scientific conclusions of medical evidence presented by the petitioner or by representative to the advisory board prior to or contemporaneously with the public hearing.
(4) Public comment period: The advisory board may provide for a public comment period. Public comment may be by written comment, verbal or both.
(a) Written comment: Any individual or association of individuals may submit written comment to the advisory board either in opposition or support of the inclusion of a medical conditions, medical treatments or diseases to the existing list of debilitating medical conditions contained under the act. All written comment shall adhere to the requirements of Subsection F of this section.
(b) Public comment: Any member of the general public may testify at the public hearing. No prior notification is required to present general non-technical statements in support of or in opposition to the petition. Any such member may also offer exhibits in connection with his testimony, so long as the exhibit is non-technical in nature and not unduly repetitious of the testimony.
I. Recording the hearing: Unless the advisory board orders otherwise, the hearing will be audio recorded. Any person, other than the advisory board, desiring a copy of the audio tapes must arrange copying with the medical cannabis program or designee at their own expense.
[7.34.2.10 NMAC - Rp, 7.34.2.10 NMAC, 2/27/2015]
7.34.2.11 ADVISORY BOARD RECOMMENDATION TO THE DEPARTMENT:
A. Advisory board recommendation: Upon final determination the advisory board shall provide to the secretary a written report of finding, which recommends either the approval or denial of the petitioner’s request. The written report of findings shall include a medical justification for the recommendation based upon the individual or collective expertise of the advisory board membership. The medical justification shall delineate between the findings of fact made by the advisory board and scientific conclusions of credible medical evidence.
B. Department final determination: The department shall notify the petitioner within 10 days of the secretary’s determination. A denial by the secretary regarding the inclusion of a medical conditions, medical treatments or diseases to the existing list of debilitating medical conditions contained under the act shall not represent a permanent denial by the department. Any individual or association of individuals may upon good cause re-petition the advisory board. All requests shall present new supporting findings of fact, or scientific conclusions of credible medical evidence not previously examined by the advisory board.
[7.34.2.11 NMAC - Rp, 7.34.2.11 NMAC, 2/27/2015]
http://164.64.110.239/nmac/parts/title07/07.034.0002.htm

No comments:
Post a Comment