
Saturday, September 16th 2017
New Mexico State Department of Health
Medical Cannabis Advisory Board
Medical Cannabis Program
PO Box 26110
Santa Fe, NM, 87502-6110
Medical Cannabis Program
PO Box 26110
Santa Fe, NM, 87502-6110
Petition: Requesting The Inclusion Of A New Medical Condition: Degenerative Neurological Disorder And Neuroprotective Applications
Table of Contents
Pg. 1 Cover Page
Pg. 2 Petition Introduction
Pg. 3 Petition Purpose and Background
Pg. 20 Relief Requested In Petition
Pg. 21 References
Pg. 27 Appendix A
Petition: Requesting The Inclusion Of A New Medical Condition: Degenerative Neurological Disorder And Neuroprotective Applications
New Mexico’s medical cannabis history started in 1978, after public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis. The New Mexico’s medical cannabis program (MCP) is the only program in the U.S. that places sole responsibility for regulation on the state’s Department of Health. Doctors must comply with state requirements for patients to be considered for applying to the medical cannabis program.
In the Lynn and Erin Compassionate Use Act, (2007) the law states; The Secretary of Health shall establish an advisory board consisting of eight practitioners representing the fields of neurology, pain management, medical oncology, psychiatry, infectious disease, family medicine and gynecology. The practitioners shall be nationally board-certified in their area of specialty and knowledgeable about the medical use of cannabis. The members shall be chosen for appointment by the Secretary from a list proposed by the New Mexico Medical Society. A quorum of the advisory board shall consist of three members. The advisory board shall:
A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis;
B. accept and review petitions to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
C. convene at least twice per year to conduct public hearings and to evaluate petitions, which shall be maintained as confidential personal health information, to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
D. issue recommendations concerning rules to be promulgated for the issuance of the registry identification cards; and
E. recommend quantities of cannabis that are necessary to constitute an adequate supply for qualified patients and primary caregivers.
First, do no harm. As an important step in becoming a doctor, medical students must take the Hippocratic Oath. And one of the promises within that oath is “first, do no harm”.
A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis;
B. accept and review petitions to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
C. convene at least twice per year to conduct public hearings and to evaluate petitions, which shall be maintained as confidential personal health information, to add medical conditions, medical treatments or diseases to the list of debilitating medical conditions that qualify for the medical use of cannabis;
D. issue recommendations concerning rules to be promulgated for the issuance of the registry identification cards; and
E. recommend quantities of cannabis that are necessary to constitute an adequate supply for qualified patients and primary caregivers.
First, do no harm. As an important step in becoming a doctor, medical students must take the Hippocratic Oath. And one of the promises within that oath is “first, do no harm”.
We have a sound law in the Lynn and Erin Compassionate Use Act, as Section 2 reads; PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
“ARTICLE 2B. LYNN AND ERIN COMPASSIONATE USE ACT
N.M. Stat. Ann. § 26-2B-2 (2009)
§ 26-2B-2. Purpose of act
The purpose of the Lynn and Erin Compassionate Use Act [26-2B-1 NMSA 1978] is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments.
HISTORY: Laws 2007, ch. 210, § 2.
EFFECTIVE DATES. --Laws 2007, ch. 210, § 12 makes the act effective July 1, 2007.”
Mosby’s Medical Dictionary states that “medical treatment” means; the management and care of a patient to combat disease or disorder. Medical treatment includes: Using prescription medications, or use of a non-prescription drug at prescription strength; and or treatment of disease by hygienic and pharmacologic remedies, as distinguished from invasive surgical procedures. Treatment may be pharmacologic, using drugs; surgical, involving operative procedures; or supportive, building the patient's strength. It may be specific for the disorder, or symptomatic to relieve symptoms without effecting a cure.(Mosby's Medical Dictionary, 9th edition.)
What is a chronic medical condition?
A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear. Harvard Medical Dictionary defines chronic as: Any condition that lasts a long time or recurs over time; chronic pain as: Pain that persists after an injury has healed or a disease is over; and chronic pain syndrome as : Long-term, severe pain that doesn't spring from an injury or illness, that interferes with daily life, and is often accompanied by other problems, such as depression, irritability, and anxiety.
A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear. Harvard Medical Dictionary defines chronic as: Any condition that lasts a long time or recurs over time; chronic pain as: Pain that persists after an injury has healed or a disease is over; and chronic pain syndrome as : Long-term, severe pain that doesn't spring from an injury or illness, that interferes with daily life, and is often accompanied by other problems, such as depression, irritability, and anxiety.
What is the meaning of debilitating?
Something that's debilitating seriously affects someone or something's strength or ability to carry on with regular activities, like a debilitating illness. Debilitating comes from the Latin word debilis, meaning "weak." That's why you'll often see the adjective used to describe illness, despite the negative reference.
Something that's debilitating seriously affects someone or something's strength or ability to carry on with regular activities, like a debilitating illness. Debilitating comes from the Latin word debilis, meaning "weak." That's why you'll often see the adjective used to describe illness, despite the negative reference.
Petition Purpose and Background
The purpose of this Petition: Requesting The Inclusion Of A New Medical Condition: Degenerative Neurological Disorder And Neuroprotective Applications
This Petition: Requesting The Inclusion Of A New Medical Condition: Degenerative Neurological Disorder And Neuroprotective Applications is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
What is a neurological disorder?
Neurological disorders are diseases of the brain, spine and the nerves that connect them. There are more than 600 diseases of the nervous system, such as brain tumors, epilepsy, Parkinson's disease and stroke as well as less familiar ones such as frontotemporal dementia.
Neurological disorders are diseases of the brain, spine and the nerves that connect them. There are more than 600 diseases of the nervous system, such as brain tumors, epilepsy, Parkinson's disease and stroke as well as less familiar ones such as frontotemporal dementia.
What is a neurodegenerative disorder?
Neurodegenerative disease is an umbrella term for a range of conditions which primarily affect the neurons in the human brain. Neurons are the building blocks of the nervous system which includes the brain and spinal cord. ... Parkinson's disease (PD) and PD-related disorders. Prion disease.
Neurodegenerative disease is an umbrella term for a range of conditions which primarily affect the neurons in the human brain. Neurons are the building blocks of the nervous system which includes the brain and spinal cord. ... Parkinson's disease (PD) and PD-related disorders. Prion disease.
Degenerative nerve diseases affect many of your body's activities, such as balance, movement, talking, breathing, and heart function. Many of these diseases are genetic. Sometimes the cause is a medical condition such as alcoholism, a tumor, or a stroke. Other causes may include toxins, chemicals, and viruses. Sometimes the cause is not known.
Degenerative nerve diseases include
Degenerative nerve diseases can be serious or life-threatening. It depends on the type. Most of them have no cure. Treatments may help improve symptoms, relieve pain, and increase mobility. (https://medlineplus.gov/degenerativenervediseases.html)
Who Should Qualify for Medical Cannabis Use?
According to Americans For Safe Access Policy Studies & Research:
Background: The most fundamental aspect of medical cannabis laws is the relationship between a patient and their physician. It is often only the physician and the patient that possess information about a patient’s health condition. However, many public officials and others who oppose medical cannabis laws often make assumptions about people’s health. The media have even fomented such inappropriate assumptions by naming a category of patients “Young Able Bodied Males,” condemning certain patients by visual assessment alone.
Findings: The health care information discussed between a patient and physician is considered private and protected under federal HIPAA laws. It is typically the purview of state medical boards to assess whether a physician has inappropriately recommended cannabis to someone who should not be qualified. Studies have shown in some medical cannabis states that the majority of patients suffer from chronic pain, an ailment that is not obviously detectable by another person. Nevertheless, police will often harass and arrest patients based on the assumption that someone is faking their illness.
Position: Medical professionals should have an unrestricted ability to recommend cannabis therapeutics and that should not be impacted by law enforcement’s perceptions.
According to Americans For Safe Access Policy Studies & Research:
Background: The most fundamental aspect of medical cannabis laws is the relationship between a patient and their physician. It is often only the physician and the patient that possess information about a patient’s health condition. However, many public officials and others who oppose medical cannabis laws often make assumptions about people’s health. The media have even fomented such inappropriate assumptions by naming a category of patients “Young Able Bodied Males,” condemning certain patients by visual assessment alone.
Findings: The health care information discussed between a patient and physician is considered private and protected under federal HIPAA laws. It is typically the purview of state medical boards to assess whether a physician has inappropriately recommended cannabis to someone who should not be qualified. Studies have shown in some medical cannabis states that the majority of patients suffer from chronic pain, an ailment that is not obviously detectable by another person. Nevertheless, police will often harass and arrest patients based on the assumption that someone is faking their illness.
Position: Medical professionals should have an unrestricted ability to recommend cannabis therapeutics and that should not be impacted by law enforcement’s perceptions.
“Qualifying medical condition” shall mean any condition for which treatment with medical cannabis would be beneficial, as determined by a patient's qualified medical professional, including but not limited to cancer, glaucoma, positive status for human immunodeficiency virus, acquired immune deficiency syndrome (AIDS), hepatitis C, amyotrophic lateral sclerosis (ALS), Crohn’s disease, Parkinson’s disease, post-traumatic stress disorder, arthritis, chronic pain, neuropathic and other intractable chronic pain, and multiple sclerosis.
“Qualifying patient” shall mean a person who has a written recommendation from a qualified medical professional for the medical use of cannabis.
Neurodegenerative Disorder And Neuroprotective Applications With Medical Cannabis
Neurodegenerative diseases are those which result mainly from dysfunction of the central nervous system (the CNS, made up of the brain and spinal cord) as a result of damage to neurons, the primary cells of this system that communicate with each other to send signals throughout the brain and body. Damage to neurons of the CNS can result in a decreased ability to send signals to the peripheral, autonomic, and enteric nervous systems, which make it possible for us to move, touch, digest, breathe, react to and sense our environment, and in general, to live.
When cells of the central nervous system are destroyed and/or not able to communicate with each other efficiently and effectively, symptoms such as cognition and memory impairment, muscle incoordination, weakness, spasticity [i.e. tight muscles and exaggerated reflexes], paralysis [i.e. an inability to move], rigidity [i.e. tight muscles], and more can occur. These symptoms can cause substantial decreases in quality of life for patients, and even death when involving reduction in function of important physiological processes like breathing and heart function. Neurodegenerative disorders are so debilitating partially because neurons are one of the few cell types with a very limited ability to regenerate (along with heart cells and skeletal muscle cells). In most cases, once neurons have been destroyed, they cannot grow back.
“If left unchecked 30 years from now, more than 12 million Americans will suffer from neurodegenerative diseases.” – Harvard Neurodiscovery Center
Examples of neurodegenerative diseases include Alzheimer’s, Parkinson’s, Huntington’s, amyotrophic lateral sclerosis(ALS, also known as “Lou Gehrig’s Disease’), spinal muscular atrophy, prion disease, and others. While multiple sclerosis (MS) has been thought to stem primarily from an autoimmune response (one in which the body starts attacking itself), there is mounting evidence that it is a disease caused by a mixture of an autoimmune and primary neurodegeneration process.
A significant amount of research on cannabis has been conducted on the plant’s potential harms in relation to brain function. However, the evidence suggests that not only are long-term, clinically significant cognitive deficits unlikely if use begins in adulthood, especially in the absence of chronic and excessive use, but cannabinoid medicine may actually prove effective in halting or reversing debilitating neurodegenerative disorders. Note: Cognitive declines as a result of use have generally been conducted using recreational users who self-report frequency of use and smoke marijuana of unknown potency and quality; studying marijuana use with alternative delivery methods (e.g. vaporization, ingestion) and controlled frequency of use with whole-plant cannabis of known ratio/concentration/potency in an adult patient population may yield vastly different results than those discovered to date which have indicated harm.
According to an article published by the Harvard Neurodiscovery Center, “If left unchecked 30 years from now, more than 12 million Americans will suffer from neurodegenerative diseases.” It is therefore imperative that the medical and scientific communities continue to extensively research any and all potentially successful therapies for these disease processes.
Cannabinoid Therapy for Neurodegenerative Diseases
Extensive research on the impact of endocannabinoid system modulation and its effects on neurodegenerative disorders has occurred in the past several years. In 2014, British Journal of Pharmacology published a review titled “The influence of cannabinoids on generic traits of neurodegeneration”, in which the authors concluded the following:
“Signalling from the CB1 and CB2 [i.e. cannabinoid] receptors are known to be involved in the regulation of Ca2+ [calcium] homeostasis [i.e. the mechanism by which systems are kept balanced], mitochondrial function [i.e. function of components of cells that produce energy], trophic [i.e. growth] support and inflammatory status… while other receptors gated [i.e. modulated/controlled] by cannabinoids… are gaining interest in their anti-inflammatory properties. Through multiple lines of evidence, this evolutionarily conserved neurosignalling system has shown neuroprotective capabilities and is therefore a potential target for neurodegenerative disorders.” While the current article briefly touches on the evidence that exists for the potential of cannabinoid therapy as treatment for neurodegenerative disorders, the BJP article will provide a more extensive overview.
“Elevation of cannabinoid receptor activity either by pharmacological blockade of the degradation of cannabinoids or by receptor agonists could be a promising strategy for slowing down the progression of brain ageing and for alleviating the symptoms of neurodegenerative disorders.” — Dr. Andras Bilkei-Gorzo
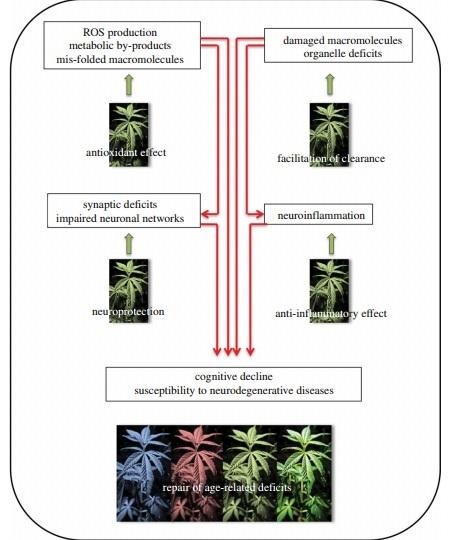
Another review published in 2012 in Philosophical Transactions of the Royal Society (source of the graphic below)discusses that cannabis may exert neuroprotective effects through mitochondrial regulation, anti-inflammatory and antioxidant (i.e. agents that prevent free radical damage) properties, and clearance of damaged cells and molecules in the brain. The author also noted that signaling of the endocannabinoid system (ECS) may decrease as people age, and therefore decreased function of the ECS may be a partial cause for age-related cognitive decline. According to the author, Dr. Andras Bilkei-Gorzo, “[E]levation of cannabinoid receptor activity either by pharmacological blockade of the degradation of cannabinoids [i.e. keeping cannabinoids active and in the brain for a longer amount of time] or by receptor agonists [i.e. receptor activation] could be a promising strategy for slowing down the progression of brain ageing and for alleviating the symptoms of neurodegenerative disorders.”
Additionally, a study published in July 2014 in the Journal of Neuroscience Research found more evidence to support the potential of cannabinoids to act as anti-inflammatory and neuroprotective agents, showing that ultralow (non-psychoactive) doses of THC were protective against “neuroinflammation-induced cognitive damage” (this study and was reviewed previously on Medical Jane).
In the image below, ROS stands for “reactive oxygen species”, which are created as intermediate products in natural physiological processes, but can cause damage to cells and tissues. “Synapses” are the junction between two neurons where signals are passed/communicated, and “organelles” are components of cells that have specific functions (e.g. mitochondria are organelles).
Conclusion
Given the highly favorable safety profile of whole-plant cannabis, and the severely debilitating symptoms caused by certain neurodegenerative diseases which could potentially be alleviated by its use, whole-plant cannabis medicine may be a safe and useful additional therapy for patients with certain neurodegenerative diseases who are finding it difficult to control their symptoms with standard therapy. Increased research on cannabinoid medicine and modulation of the endocannabinoid system in relation to neurodegeneration has the potential to lead to novel therapies which may help to prevent progression, and potentially initiation, of these diseases.
For information on how you can advocate, expectations, and safety in considering whole-plant medical cannabis use, click here.
(https://www.medicaljane.com/2014/11/11/cannabis-classroom-neurodegenerative-disease-and-medical-marijuana/)
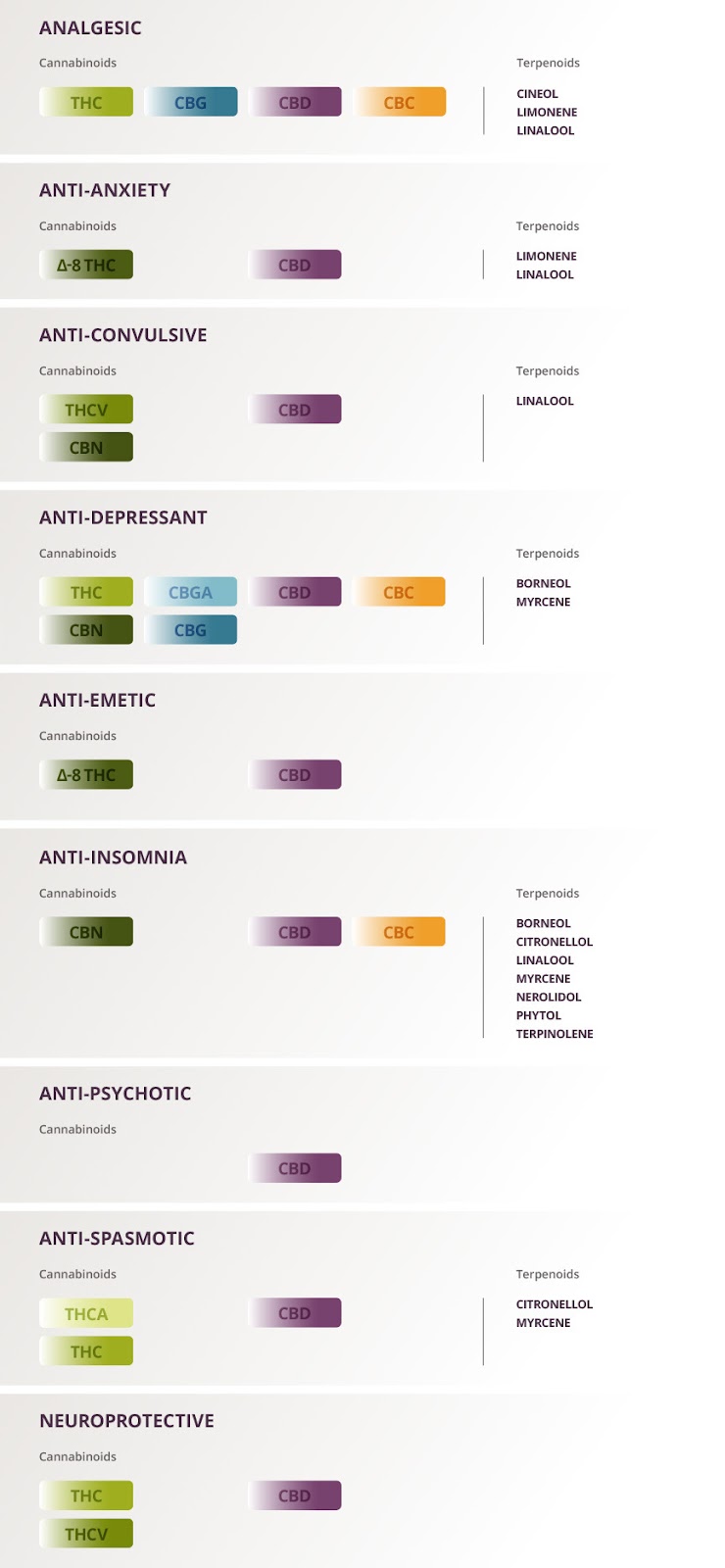
Beneficial Cannabinoids and Terpenoids Useful for Treating Degenerative Neurological Disorder And Neuroprotective Applications
The cannabis plant offers a plethora of therapeutic benefits and contains cannabinoids and terpenoid compounds that are useful for treating the symptoms of Degenerative Neurological Disorder And Neuroprotective Applications. While most of the ongoing research focuses on CBD and THC, the following list also denotes which cannabinoids and terpenoids work synergistically with each other for possible therapeutic benefit. It may be beneficial to seek out strains that contain these cannabinoids and terpenoids.
(See References Section For Sources Cited Listed As: References )
FINDINGS: EFFECTS OF CANNABIS ON NEUROLOGICAL DISORDERS
Research has shown that cannabis possesses neuroprotective effects, which in turn support the health of the brain, spinal cord and nerves, and help in preventing and limiting the progression of various neurological disorders. The major cannabinoids found in cannabis, including cannabidiol (CBD) and tetrahydrocannabinol (THC), have both shown they can help protect neurons, modulate the inflammatory response and encourage neuroregeneration (Lafuente, et al., 2011) (Kubajewska & Constantinescu, 2010) (Croxford, et al., 2008). Amyotrophic Lateral Sclerosis (ALS) The cannabinoids in cannabis have shown they are capable of delaying the onset of ALS, prolonging neuron survival and slowing the progression of the disease (Bilsland, et al., 2006) (Carter, Abood, Aggarwal & Weiss, 2010) (Raman, et al., 2004). CBD specifically has been found to significantly slow the onset of ALS (Weydt, et al., 2005). Cannabis can also help with managing the pain, appetite loss, depression, sleeping problems, spasticity and drooling associated with ALS (Amtmann, et al., 2004) (Carter, Abood, Aggarwal & Weiss, 2010). Epilepsy In numerous studies, CBE has demonstrated the ability to reduce or even eliminate seizures (Blair, Deshpande & DeLorenzo, 2015) (Rosenberg, Tsien, Whalley & Devinsky, 2015) (Szaflarski & Bebin, 2014) (Devinsky, et al., 2014). Migraine Through their activation of the CB1 and CB2, cannabinoids effectively inhibits the pain response caused by migraines (Akerman, Holland, Lasalandra & Goardsby, 2013) (Baron, 2015) (Greco, et al., 2014).Multiple Sclerosis (MS) Cannabis’ cannabinoids slow the neurodegenerative process of multiple sclerosis by helping to regulate the body’s immune system, modulating its inflammatory response and encouraging neuroregeneration (Kubajewska & Constantinescu, 2010) (Croxford, et al., 2008). One study showed that cannabinoids reduced the damage to myelin caused from inflammation, thereby offering neuroprotection (Pryce, et al., 2003). Another found that cannabinoids reduced neurological disability, improved motor coordination and limited the progression of the MS in animals with a model of multiple sclerosis (de Lago, et al., 2012). Parkinson’s Disease Studies show that cannabis’ neuroprotective effects can slow the progression of Parkinson’s. Its cannabinoids suppress excitotoxicity, glial activation and oxidative injury that lead to neuron degeneration. They improve the mitochondria function and the clearance of cellular debris, which also supports neuron health (More & Choi, 2015) (Garcia-Arencibia, Garcia & Fernandez-Ruiz, 2009) (Lastres-Becker & Fernandez-Ruiz, 2006). CBD has also shown to support the health of neural cells mitochondria (da Silva, et al., 2014) (Zuardi, 2008). Peripheral Neuropathy Cannabis effectively reduces neuropathic pain (Jensen, Chen, Furnish & Wallace, 2015) (Baron, 2015) (McDonough, McKenna, McCreary & Downer, 2014). Cannabis-based medicines have even shown they can reduce chronic neuropathic pain that had previously proven refractory to other treatments (Boychuk, Goddard, Mauro & Orellana, 2015). Prion Diseases CBD has shown to protect neurons against prion toxicity and therefore reduced the risk of prion diseases, a group of rare degenerative brain disorders (Dirikoc, et al., 2007). Spinal Cord Injury Cannabis’ cannabinoids limit neurological damage caused by a spinal cord injury if administered shortly after the traumatic event. The cannabinoids reduce the proinflammatory cytokines and delay the atrophy and degeneration of neurons and thereby protect the white matter and myelin sheath surrounding the cord and nerves (Arevalo-Martin, Garcia-Ovejero & Molina-Holgado, 2010) (Latini, et al., 2014) (Arevalo-Martin, Garcia-Ovejero & Molina-Holgado, 2010) (Arevalo-Martin, et al., 2012). An animal trial have found the administration of cannabinoids shortly after a spinal cord injury caused an improvement in locomotor functional recovery (Kwiatkoski, Guimaraes & Del-Bel, 2012). In addition, cannabis has found to be among the most effective pain relief treatments for people with spinal cord injuries (Wilsey, et al., 2013) (Heutink, Post, Wollaars & van Asbeck, 2011). Stroke Cannabinoids reduce infarct volume and improving functional outcome following strokes (England, Hind, Rasid & O’Sullivan, 2015). When administered shortly after a stroke, CBD specifically protects neurons and astrocytes from damage, and therefore leads to improved functional, histological, biochemical, and neurobehavior recovery (Lafuente, et al., 2011). Tourette Syndrome Cannabis effectively suppresses tics and improves behavioral problems associated with Tourette syndrome (Muller-Vahl, 2013) (Muller-Vahl, et al., 2002). Tumors of the Brain and Spinal Cord CBD has shown it has anti-tumor properties, with one study showing it significantly inhibited the growth of cancer cells (Massi, et al., 2004).
STATES THAT HAVE APPROVED MEDICAL CANNABIS FOR NEUROLOGICAL DISORDERS
No states include “neurological disorders” on their list of approved conditions for medical cannabis, despite the Federal Government owning the Patent providing it should be use for it. Pennsylvania and West Virginia allow medicinal cannabis for “damage to the nervous tissue of the spinal cord with objective neurological indication of intractable spasticity.” Additionally, many other states allow medical marijuana for the treatment of specific neurological disorders. For example, Arizona, Arkansas, Connecticut, Delaware, Florida, Georgia, Maine, Massachusetts, Michigan, Minnesota, New Hampshire, New Jersey, New Mexico, New York, North Dakota, Ohio, Pennsylvania and West Virginia have approved medical marijuana for the treatment of ALS. Alabama, Connecticut, Delaware, Florida, Georgia, Iowa, Louisiana, Maine, Mississippi, Missouri, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Pennsylvania, South Carolina, Texas, Utah, Virginia, West Virginia, Wisconsin, and Wyoming have approved medical marijuana for the treatment of either epilepsy or seizure disorders. California and Illinois have specifically approved medical marijuana for the treatment of migraines. Arkansas, Montana, New Mexico, New York, Pennsylvania and West Virginia have approved medical marijuana for the treatment of neuropathy. New Hampshire, New Mexico, New York, North Dakota, Ohio and Pennsylvania have approved medical marijuana specifically for the treatment of spinal cord injuries. Arkansas, Illinois, Minnesota and Ohio have approved medical marijuana specifically for the treatment of Tourette syndrome. Connecticut, Florida, Georgia, Illinois, Maine, Massachusetts, New Hampshire, New Mexico, New York, Ohio, Pennsylvania and West Virginia have approved medical marijuana for the treatment of Parkinson’s disease. Alaska, Connecticut, Florida, Georgia, Illinois, Maine, Massachusetts, New Hampshire, New Jersey, New Mexico, New York, Ohio, Pennsylvania, Vermont and West Virginia allow medical marijuana for the treatment of multiple sclerosis. Alaska, Arizona, Arkansas, California, Colorado, Connecticut, Delaware, Florida, Georgia, Hawaii, Illinois, Louisiana, Maine, Massachusetts, Michigan, Minnesota, Montana, Nevada, New Hampshire, New Jersey, New Mexico, New York, North Dakota, Ohio, Oregon, Pennsylvania, Rhode Island, Vermont, Washington and West Virginia legally allow medical marijuana for the treatment of cancer, including tumors. Currently, no states have approved medical marijuana specifically for the treatment of stroke. However, in Washington D.C., any condition can be approved for medical marijuana as long as a DC-licensed physician recommends the treatment. Plus, various other states will consider allowing medical marijuana to be used for the treatment of neurological disorders with the recommendation from a physician. These states include: California (any debilitating illness where the medical use of marijuana has been recommended by a physician), Connecticut (other medical conditions may be approved by the Department of Consumer Protection), Massachusetts (other conditions as determined in writing by a qualifying patient’s physician), Nevada (other conditions subject to approval), Oregon (other conditions subject to approval), Rhode Island (other conditions subject to approval), and Washington (any “terminal or debilitating condition”). In addition, various states have approved medical marijuana for symptoms commonly associated with neurological disorders. Many states have approved medical marijuana specifically to treat chronic pain. These states include: Alaska, Arizona, California, Colorado, Delaware, Hawaii, Maine, Maryland, Michigan, Montana, New Mexico, Ohio, Oregon, Pennsylvania, Rhode Island and Vermont. The states of Nevada, New Hampshire, North Dakota, Montana, Ohio, Vermont and West Virginia allow medical marijuana to treat “severe pain.” The states of Arkansas, Minnesota, Ohio, Pennsylvania and Washington have approved cannabis for the treatment of “intractable pain.” Alaska, Arizona, Arkansas, California, Colorado, Delaware, Hawaii, Louisiana, Maryland, Michigan, Minnesota, Montana, Nevada, New Hampshire, North Dakota, Ohio, Oregon, Pennsylvania (intractable seizures), Rhode Island, Tennessee(intractable seizures), Vermont, Washington and West Virginia have approved medical marijuana to treat seizures. Arizona, Arkansas, California, Colorado, Delaware, Florida, Hawaii, Maryland, Michigan, Minnesota, Montana, Nevada, New Hampshire, Oregon, Rhode Island and Washington have approved medical marijuana for the treatment of spasms.
RECENT STUDIES ON CANNABIS’ EFFECT ON NEUROLOGICAL DISORDERS
- Cannabis delays the onset of ALS and slow the progression of the disease. Cannabis and amyotrophic lateral sclerosis: hypothetical and practical applications, and a call for clinical trials.(http://journals.sagepub.com/doi/pdf/10.1177/1049909110369531)
- CBD-enriched cannabis reduced seizure frequency in 85% of children and caused complete seizure freedom in 14% of children. Perceived efficacy of cannabidiol-enriched cannabis extracts for treatment of pediatric epilepsy: A potential role for infantile spasms and Lennox-Gastaut syndrome. (http://www.epilepsybehavior.com/article/S1525-5050(15)00157-2/fulltext)
- Cannabinoids administered shortly following spinal cord injury limits damage. Early endogenous activation of CB1 and CB2 receptors after spinal cord injury is a protective response involved in spontaneous recovery. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3496738/)
- Smoking cannabis significantly improved tremors, rigidity and bradykinesia in Parkinson’s disease patients. Cannabis (medical marijuana) treatment for motor and non-motor symptoms of Parkinson disease: an open-label observational study.(http://journals.lww.com/clinicalneuropharm/pages/articleviewer.aspx?year=2014&issue=03000&article=00001&type=abstract)
- CBD administered shortly following an ischemic event increased the recovery of electrical activity in the brain by about 50% and reduced seizures by 50%. Neuroprotective effects of the nonpsychoactive cannabinodi cannabidiol in hypoxic-ischemic newborn piglets. (http://www.nature.com/pr/journal/v64/n6/full/pr2008260a.html)
- Cannabinoids reduced neurological disability and the progression of multiple sclerosis in mice. Cannabinoids ameliorate disease progression in a model of multiple sclerosis in mice, acting preferentially through CB1 receptor-mediated anti-inflammatory effects.(http://www.sciencedirect.com/science/article/pii/S0028390812000500)
- Four weeks of cannabis treatment significantly improved spasms in MS patients. A randomized double-blind-placebo-controlled, parallel-group, enriched-design study of nabiximols* (Sativex(®)), as add-on therapy, in subjects with refractory spasticity caused by multiple sclerosis. (http://onlinelibrary.wiley.com/wol1/doi/10.1111/j.1468-1331.2010.03328.x/full)
- Cannabis significantly improves neuropathic pain that was refractory to other treatments.The effectiveness of cannabinoids in the management of chronic nonmalignant neuropathic pain: a systematic review. (https://goo.gl/R28LWD)
- Six weeks of cannabis treatment reduced tics in patients with Tourette’s syndrome.Cannabinoids reduce symptoms of Tourette’s syndrome.(http://www.tandfonline.com/doi/pdf/10.1517/14656566.4.10.1717?needAccess=true)
(See References Section For Sources Cited Listed As: References I)
Cannabinoids as antioxidants and neuroprotectants
Cannabinoids have been found to have antioxidant properties, unrelated to NMDA receptor antagonism. This new found property makes cannabinoids useful in the treatment and prophylaxis of wide variety of oxidation associated diseases, such as ischemic, age-related, inflammatory and autoimmune diseases. The cannabinoids are found to have particular application as neuroprotectants, for example in limiting neurological damage following ischemic insults, such as stroke and trauma, or in the treatment of neurodegenerative diseases, such as Alzheimer's disease, Parkinson's disease and HIV dementia. Nonpsychoactive cannabinoids, such as cannabidiol, are particularly advantageous to use because they avoid toxicity that is encountered with psychoactive cannabinoids at high doses useful in the method of the present invention. A particular disclosed class of cannabinoids useful as neuroprotective antioxidants is formula (I) wherein the R group is independently selected from the group consisting of H, CH.sub.3, and COCH.sub.3. ##STR1##
United States Patent 6,630,507
Hampson , et al. October 7, 2003
Hampson , et al. October 7, 2003
The Patent Research Show That:
1. A method of treating diseases caused by oxidative stress, comprising administering a therapeutically effective amount of a cannabinoid that has substantially no binding to the NMDA receptor to a subject who has a disease caused by oxidative stress.
2. The method of claim 1, wherein the cannabinoid is nonpsychoactive.
3. The method of claim 2, wherein the cannabinoid has a volume of distribution of 10 L/kg or more.
4. The method of claim 1, wherein the cannabinoid is not an antagonist at the NMDA receptor.
5. The method of claim 1, wherein the cannabinoid is: ##STR22##
where R is H, substituted or unsubstituted alkyl, carboxyl, alkoxy, aryl, aryloxy, arylalkyl, halo or amino.
6. The method of claim 5, wherein R is H, substituted or unsubstituted alkyl, carboxyl or alkoxy.
7. The method of claim 2, wherein the cannabinoid is: ##STR23##
where A is cyclohexyl, substituted or unsubstituted aryl, or ##STR24## but not a pinene; R.sub.1 is H, substituted or unsubstituted alkyl, or substituted or unsubstituted carboxyl; R.sub.2 is H, lower substituted or unsubstituted alkyl, or alkoxy; R.sub.3 is of H, lower substituted or unsubstituted alkyl, or substituted or unsubstituted carboxyl; R.sub.4 is H, hydroxyl, or lower substituted or unsubstituted alkyl; and R.sub.5 is H, hydroxyl, or lower substituted or unsubstituted alkyl.
8. The method of claim 7, wherein R.sub.1 is lower alkyl, COOH or COCH.sub.3 ; R.sub.2 is unsubstituted C.sub.1 -C.sub.5 alkyl, hydroxyl, methoxy or ethoxy; R.sub.3 is H, unsubstituted C.sub.1 -C.sub.3 alkyl, or COCH.sub.3 ; R.sub.4 is hydroxyl, pentyl, heptyl, or diemthylheptyl; and R.sub.5 is hydroxyl or methyl.
9. The method of claim 1, wherein the cannabinoid is: ##STR25##
where R.sub.1, R.sub.2 and R.sub.3 are independently H, CH.sub.3, or COCH.sub.3.
10. The method of claim 9, wherein the cannabinoid is: ##STR26##
where: a) R.sub.1 =R.sub.2 =R.sub.3 =H; b) R.sub.1 =R.sub.3 =H, R.sub.2 =CH.sub.3 ; c) R.sub.1 =R.sub.2 =CH.sub.3, R.sub.3 =H; d) R.sub.1 =R.sub.2 =COCH.sub.3, R.sub.3 =H; or e) R.sub.1 =H, R.sub.2 =R.sub.3 =COCH.sub.3.
11. The method of claim 2, wherein the cannabinoid is: ##STR27##
where R.sub.19 is H, lower alkyl, lower alcohol, or carboxyl; R.sub.20 is H or OH; and R.sub.21 -R.sub.25 are independently H or OH.
12. The method of claim 11, wherein R.sub.19 is H, CH.sub.3, CH.sub.2 OH, or COOH, and R.sub.20 -R.sub.24 are independently H or OH.
13. The method of claim 2, wherein the cannabinoid is: ##STR28##
where R.sub.19 and R.sub.20 are H, and R.sub.26 is alkyl.
14. The method of claim 10, wherein the cannabinoid is cannabidiol.
15. A method of treating an ischemic or neurodegenerative disease in the central nervous system of a subject, comprising administering to the subject a therapeutically effective amount of a cannabinoid, where the cannabinoid is ##STR29##
where R is H, substituted or unsubstituted alkyl, carboxyl, alkoxy, aryl, aryloxy, arylalkyl, halo or amino.
16. The method of claim 15, wherein the cannabinoid is not a psychoactive cannabinoid.
17. The method of claim 15 where the ischemic or neurodegenerative disease is an ischemic infarct, Alzheimer's disease, Parkinson's disease, and human immunodeficiency virus dementia, Down's syndrome, or heart disease.
18. A method of treating a disease with a cannabinoid that has substantially no binding to the NMDA receptor, comprising determining whether the disease is caused by oxidative stress, and if the disease is caused by oxidative stress, administering the cannabinoid in a therapeutically effective antioxidant amount.
19. The method of claim 18, wherein the cannabinoid has a volume of distribution of at least 1.5 L/kg and substantially no activity at the cannabinoid receptor.
20. The method of claim 19, wherein the cannabinoid has a volume of distribution of at least 10 L/kg.
21. The method of claim 1, wherein the cannabinoid selectively inhibits an enzyme activity of 5- and 15-lipoxygenase more than an enzyme activity of 12-lipoxygenase.
22. A method of treating a neurodegenerative or ischemic disease in the central nervous system of a subject, comprising administering to the subject a therapeutically effective amount of a compound selected from any of the compounds of claims 9 through 13.
23. The method of claim 22 where the compound is cannabidiol.
24. The method of claim 22, wherein the ischemic or neurodegenerative disease is an ischemic infarct, Alzheimer's disease, Parkinson's disease, and human immunodeficiency virus dementia, Down's syndrome, or heart disease.
25. The method of claim 24 wherein the disease is an ischemic infarct.
26. The method of claim 1, wherein the cannabinoid is not an antagonist at the AMPA receptor.
U.S. Patent Documents Pertaining to This Patent
December 1942
|
Adams
| |
October 1989
|
Mechoulam et al.
| |
July 1993
|
Stoss et al.
| |
February 1994
|
Kloog et al.
| |
July 1995
|
Mechoulam et al.
| |
October 1995
|
Mitchell et al.
| |
April 1996
|
Ghio et al.
| |
May 1996
|
Mechoulam et al.
| |
July 1996
|
Mechoulam et al.
| |
June 1997
|
Mechoulam et al.
| |
December 1997
|
Malfroy-Camine et al.
| |
June 2002
|
Feldmann et al.
|
Foreign Patent Documents
427518
|
May 1991
|
EP
| |||
576357
|
Dec 1993
|
EP
| |||
656354
|
Jun 1995
|
EP
| |||
658546
|
Jun 1995
|
EP
| |||
WO9305031
|
Mar 1993
|
WO
| |||
WO9412667
|
Jun 1994
|
WO
| |||
WO9612485
|
May 1996
|
WO
| |||
WO9618600
|
Jun 1996
|
WO
| |||
WO9719063
|
May 1997
|
WO
| |||
99/53917
|
Oct 1999
|
WO
|
Other References For This Patent
Windholz et al., The Merck Index, Tenth Edition (1983) p. 241, abstract No. 1723.* .
Mechoulam et al., "A Total Synthesis of d1-.DELTA..sup.1 -Tetrahydrocannabinol, the Active Constituent of Hashish.sup.1," Journal of the American Chemical Society, 87:14:3273-3275 (1965). .
Mechoulam et al., "Chemical Basis of Hashish Activity," Science, 18:611-612 (1970). .
Ottersen et al., "The Crystal and Molecular Structure of Cannabidiol," Acta Chem. Scand. B 31, 9:807-812 (1977). .
Cunha et al., "Chronic Administration of Cannabidiol to Healthy Volunteers and Epileptic Patients.sup.1," Pharmacology, 21:175-185 (1980). .
Consroe et al., "Acute and Chronic Antiepileptic Drug Effects in Audiogenic Seizure-Susceptible Rats," Experimental Neurology, Academic Press Inc., 70:626-637 (1980). .
Turkanis et al., "Electrophysiologic Properties of the Cannabinoids," J. Clin. Pharmacol., 21:449S-463S (1981). .
Carlini et al., "Hypnotic and Antielpileptic Effects of Cannabidiol," J. Clin. Pharmacol., 21:417S-427S (1981). .
Karler et al., "The Cannabinoids as Potential Antiepileptics," J. Clin. Pharmacol., 21:437S-448S (1981). .
Consroe et al., "Antiepileptic Potential of Cannabidiol Analgos," J. Clin. Pharmacol., 21:428S-436S (1981). .
Colasanti et al., "Ocular Hypotension, Ocular Toxicity,a nd Neurotoxicity in Response to Marihuana Extract and Cannabidiol," Gen Pharm., Pergamon Press Ltd., 15(6):479-484 (1984). .
Colasanti et al., "Intraocular Pressure, Ocular Toxicity and Neurotoxicity after Administration of Cannabinol or Cannabigerol," Exp. Eye Res., Academic Press Inc., 39:251-259 (1984). .
Volfe et al., "Cannabinoids Block Release of Serotonin from Platelets Induced by Plasma frm Migraine Patients," Int. J. Clin. Pharm. Res., Bioscience Ediprint Inc., 4:243-246 (1985). .
Agurell et al., "Pharmacokinetics and Metabolism of .DELTA..sup.1 -Tetrahydrocannabinol and Other Cannabinoids with Emphasis on Man*," Pharmacological Reviews, 38(1):21-43 (1986). .
Karler et al., "Different Cannabinoids Exhibit Different Pharmacological and Toxicological Properties,"NIDA Res. Monogr., 79:96-107 (1987). .
Samara et al., "Pharmacokinetics of Cannabidiol in Dogs," Drug Metabolism and Disposition, 16(3):469-472 (1988). .
Choi, "Glutamate Neurotoxicity and Diseases of the Nervous System," Neuron, Cell Press, 1:623-634 (1988). .
Eshhar et al., "Neuroprotective and Antioxidant Activities of HU-211, A Novel NMDA Receptor Antagonist," European Journal of Pharmacology, 283:19-29 (1995). .
Skaper et al., "The ALIAmide Palmitoylethanolamide and Cannabinoids, but not Anandamide, are Protective in a Delayed Postglutamate Paradigm of Excitotoxic Death in Cerebellar Granule Neurons," Neurobiology, Proc. Natl. Acad. Sci. USA, 93:3984-3989 (1996). .
Alonso et al., "Simple Synthesis of 5-Substituted Resorcinols: A Revisited Family of Interesting Bioactive Molecules," J. Org. Chem., American Chemical Society, 62(2):417-421 (1997). .
Combes et al. "A Simple Synthesis of the Natural 2,5-Dialkylresorcinol Free Radical Scavenger Antioxidant: Resorstation," Synthetic Communications, Marcel Dekker, Inc., 27(21):3769-3778 (1997). .
Shohami et al., "Oxidative Stress in Closed-Head Injury: Brain Antioxidant Capacity as an Indicator of Functional Outcome," Journal of Cerebral Blood Flow and Metabolism, Lippincott-Raven Publishers, 17(10):1007-1019 (1997). .
Zurier et al., "Dimethylheptyl-THC-11 OIC Acid," Arthritis & Rheumatism, 41(1):163-170 (1998). .
Hampson et al., "Dual Effects of Anandamide on NMDA Receptor-Mediated Responses and Neurotransmission," Journal of Neurochemistry, Lippincott-Raven Publishers, 70(2):671-676 (1998). .
Hampson et al., "Cannabidiol and (-).DELTA..sup.9 -tetrahydrocannabiono are Neuroprotective Antioxidants," Medical Sciences, Proc. Natl. Acad. Sci. USA, 8268-8273 (1998)..
|
Primary Examiner: Weddington; Kevin E.
Attorney, Agent or Firm: Klarquist Sparkman, LLP
A number of experts, including CNN’s chief medical correspondent Dr. Sanjay Gupta, have noted the contradiction between federal marijuana law and the government’s patent.
“The United States government owns a patent on cannabis as a medical application… So we have a patent through our Department of HHS on cannabis as a therapeutic and we also schedule it as a Schedule I.”
Rules, Regulations, & Policy Solution For Petition: Requesting The Inclusion Of A New Medical Condition: Degenerative Neurological Disorder And Neuroprotective Applications
The approval of this Petition: Requesting The Inclusion Of A New Medical Condition: Degenerative Neurological Disorder And Neuroprotective Applications, that is being provided to the state Department of Health Medical Cannabis Program so the advisory board can review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis with the Lynn and Erin Compassionate Use Act.
The approval of this petition would bring the Department of Health in compliance with the intent of the law and uphold the spirit of the Lynn and Erin Compassionate Use Act, 2007. Fulfilling both;“ Section 2. PURPOSE OF ACT.--The purpose of the Lynn and Erin Compassionate Use Act is to allow the beneficial use of medical cannabis in a regulated system for alleviating symptoms caused by debilitating medical conditions and their medical treatments” And Section 6. ADVISORY BOARD CREATED--DUTIES: The advisory board shall: A. review and recommend to the department for approval additional debilitating medical conditions that would benefit from the medical use of cannabis.” New Mexico’s medical cannabis history started in 1978. After public hearings the legislature enacted H.B. 329, the nation’s first law recognizing the medical value of cannabis...the first law.
References
Understanding medical cannabis.Elemental Wellness Center, 2014 Jul.
References I:
Akerman, S., Holland, P.R., Lasalandra, M.P. and Goadsby, PJ. (2013, September). Endocannabinoids in the brainstem modulate dural trigeminovascular nociceptive traffic via CB1 and “triptan” receptors: implications in migraine. Journal of Neuroscience, 33(37), 14869-77. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3771033/. Alvarez, F.J., Lafuente, H., Rey-Santano, M.C., Mielgo, V.E., Gastiasoro, E., Rueda, M., Pertwee, R.G., Castillo, A.I., Romero, J., and Martinez-Orgado, J. (2008). Neuroprotective effects of the nonpsychoactive cannabinoid cannabidiol in hypoxic-ischemic newborn piglets. Pediatric Research, 64, 653-648. Retrieved from http://www.nature.com/pr/journal/v64/n6/full/pr2008260a.html. Amtmann, D., Weydt, P., Johnson, K.L., Jensen, M.P., and Carter, G.T. (2004). Survey of cannabis use in patients with amyotrophic lateral sclerosis. The American Journal of Hospice and Palliative Care, 21(2), 94-104. Retrieved from http://journals.sagepub.com/doi/pdf/10.1177/104990910402100206. Arevalo-Martin, A., Garcia-Ovejero, D., and Molina-Holgado, E. (2010, May). The endocannabinoid 2-arachidonoylglycerol reduces lesion expansion and white matter damage after spinal cord injury. Neurobiology of Disease, 38(2), 304-12. Retrieved from http://www.sciencedirect.com/science/article/pii/S0969996110000409. Arevalo-Martin, A., Garcia-Ovejero, D., Sierra, Palomares, Y., Paniagua-Torija, B., Gonzalez-Gil, I., Oretega-Gutierrez, S., and Molina-Holgado, E. (2012). Early endogenous activation of CB1 and CB2 receptors after spinal cord injury is a protective response involved in spontaneous recovery. PLOS One, 7(11), e49057. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3496738/. Baron, E.P. (2015, June). Comprehensive Review of Medicinal Marijuana, Cannabinoids, and Therapeutic Implications in Medicine and Headache: What a Long Strange Trip It’s Been… Headache, 55(6), 885-916. Retrieved from http://onlinelibrary.wiley.com/wol1/doi/10.1111/head.12570/full. Bilsland, L.G., Dick, J.R., Pryce, G., Petrosino, S., Di Marzo, V., Baker, D., and Greensmith, L. (2006). Increasing cannabinoid levels by pharmacological and genetic manipulation delay disease progression in SOD1 mice. The FASEB Journal, 20(7), 1003-1005. Retrieved from http://www.fasebj.org/content/20/7/1003.long. Blair, R.E., Deshpande, L.S., and DeLorenzo, R.J. (2015, September). Cannabinoids: is there a potential treatment role in epilepsy? Expert Opinion on Pharmacology, 16(13), 1911-4. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4845642/. Blázquez, C., Chiarlone, A., Bellocchio, L., Resel, E., Pruunsild, P., García-Rincón, D., Sendtner, M., Timmusk, T., Lutz, B., Galve-Roperh, I., and Guzmán, M. (2015). The CB1 cannabinoid receptor signals striatal neuroprotection via a PI3K/Akt/mTORC1/BDNF pathway. Cell Death and Differentiation, 22(10), 1618–1629. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4563779/. Boychuk, D.G., Goddard, G., Mauro, G., and Orellana, M.R. (2015, Winter). The effectiveness of cannabinoids in the management of chronic nonmalignant neuropathic pain: a systematic review. Journal of Oral & Facial Pain and Headache, 29(1), 7-14. Retrieved from https://goo.gl/R28LWD. Carter, G.T., Abood, M.E., Aggarwal, S.K and Weiss, M.D. (2010). Cannabis and amyotrophic lateral sclerosis: hypothetical and practical applications, and a call for clinical trials. American Journal of Hospice & Palliative Medicine, 27(5), 347-356. Retrieved from http://journals.sagepub.com/doi/pdf/10.1177/1049909110369531. Castelli, M.P., Madeddu, C., Casti, A., Casu, A., Casti, P., Scherma, M., Fattore, L., Fadda, P., and Ennas, M.G. (2014). Δ9-Tetrahydrocannabinol Prevents Methamphetamine-Induced Neurotoxicity. PLoS ONE, 9(5), e98079. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4028295/. Chen, J., Lee, C.T., Errico, S., Deng, X., Cadet, J.L., and Freed, W.J. (2005). Protective effects of Δ9-tetrahydrocannabinol against N-methyl-D-aspartate-induced AF5 cell death. Brain Research. Molecular Brain Research, 134(2), 215–225. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1824211/. Croxford, J.L., Pryce, G., Jackson, S.J., Ledent, C., Giovannoni, G., Pertwee, R.G., Yamamura, T., and Baker, D. (2008, January). Cannabinoid-mediated neuroprotection, not immunosuppression, may be more relevant to multiple sclerosis. Journal of Neuroimmunology, 193(1-2), 120-9. Retrieved from http://www.jni-journal.com/article/S0165-5728(07)00396-7/fulltext. da Silva, V.K., de Freitas, B.S., da Silva Dornelles, A., Nery, L.R., Falavigna, L., Ferreira, R.D., Bogo, M.R., Hallak, J.E., Zuardi, A.W., Crippa, J.A., and Schroder, N. (2014, February). Cannabidiol normalizes caspase 3, synaptophysin, and mitochondrial fission protein DNM1L expression levels in rats with brain iron overload: implications for neuroprotection. Molecular Neurobiology, 49(1), 222-33. Retrieved from http://link.springer.com/article/10.1007%2Fs12035-013-8514-7. de Lago, E., Moreno-Martet, M., Cabranes, A., Ramos, J.A., and Fernandez-Ruiz, J. (2012, June). Cannabinoids ameliorate disease progression in a model of multiple sclerosis in mice, acting preferentially through CB1 receptor-mediated anti-inflammatory effects. Neuropharmacology, 62(7), 2299-308. Retrieved from http://www.sciencedirect.com/science/article/pii/S0028390812000500. Devinsky, O., Cilio, M.R., Cross, H., Fernandez-Ruiz, J., French, J., Hill, C., Katz, R., Di Marzo, V., Jutras-Aswad, D., Notcutt, W.G., Martinez-Orgado, J., Robson, P.J., Rohrback, B.G., Thiele, E., Whalley, B., and Friedman, D. (2014, June). Cannabidiol: pharmacology and potential therapeutic role in epilepsy and other neuropsychiatric disorders. Epilepsia, 55(6), 791-802. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4707667/. Dirikoc, S., Priola, S.A., Marella, M., Zsurger, N., and Chabry, J. (2007, September 5). Nonpsychoactive cannabidiol prevents prion accumulation and protects neurons against prion toxicity. Journal of Neuroscience, 27(36), 9537-44. Retrieved from http://www.jneurosci.org/content/27/36/9537.long. Disorder Index. (n.d.). National Institute of Neurological Disorders and Stroke. Retrieved from http://www.ninds.nih.gov/disorders/disorder_index.htm#A. England, T.J., Hind, W.H., Rasid, N.A., and O’Sullivan, S.E. (2015, March). Cannabinoids in experimental stroke: a systematic review and meta-analysis. Journal of Cerebral Blood Flow and Metabolism, 35(3), 348-58. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4348386/. Fernandez-Ruiz, J., Sagredo, O., Pazos, M.R., Garcia, C., Pertwee, R., Mechoulam, R., and Martinez-Orgado, J. (2013, February). Cannabidiol for neurodegenerative disorders: important new clinical applications for this phytocannabinoid? British Journal of Clinical Pharmacology, 75(2), 323-33. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3579248/. Fernández-Ruiz, J., Romero, J., Velasco, G., Tolon, R.M., Ramos, J.A., and Guzman, M. (2007, January). Cannabinoid CB2 receptor: a new target for controlling neural cell survival. Trends in Pharmaceutical Sciences, 28(1), 39-45. Retrieved from http://www.cell.com/trends/pharmacological-sciences/fulltext/S0165-6147(06)00267-7. Fernández-Ruiz, J., Moro, M. A., & Martínez-Orgado, J. (2015). Cannabinoids in Neurodegenerative Disorders and Stroke/Brain Trauma: From Preclinical Models to Clinical Applications. Neurotherapeutics, 12(4), 793–806. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4604192/. Fernández-Ruiz, J., Moreno-Martet, M., Rodríguez-Cueto, C., Palomo-Garo, C., Gómez-Cañas, M., Valdeolivas, S., Guaza, C., Romero, J., Guzman, M., Mechoulam, R., and Ramos, J. A. (2011). Prospects for cannabinoid therapies in basal ganglia disorders. British Journal of Pharmacology, 163(7), 1365–1378. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3165947/. Fishbein, M., Gov, S., Assaf, F., Gafni, M., Keren, O., and Sarne, Y. (2012, September). Long-term behavioral and biochemical effects of an ultra-low dose of Δ9-tetrahydrocannabinol (THC): neuroprotection and ERK signaling. Experimental Brain Research, 221(4), 437-48. Retrieved from http://link.springer.com/article/10.1007%2Fs00221-012-3186-5. Garcia-Arencibia, M., Garcia, C., and Fernandez-Ruiz, J. (2009, December). Cannabinoids and Parkinson’s disease. CNS & Neurological Disorders Drug Targets, 8(6), 432-9. Retrieved from http://www.eurekaselect.com/93569/article. Greco, R., Mangione, A.S., Sandrini, G., Nappi, G. and Tassorelli, C. (2014, March). Activation of CB2 receptors as a potential therapeutic target for migraine: evaluation in an animal model. The Journal of Headache and Pain, 15, 14. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3995520/. Hamelink, C., Hampson, A., Wink, D.A., Eiden, L.E., and Eskay, R.L. (2005). Comparison of Cannabidiol, Antioxidants, and Diuretics in Reversing Binge Ethanol-Induced Neurotoxicity. The Journal of Pharmacology and Experimental Therapeutics, 314(2), 780–788. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4183207/. Hampson, A.J., Grimaldi, M., Lolic, M., Wink, D., Rosenthal, R., and Axelrod, J. (2000). Neuroprotective antioxidants from marijuana. Annals of the New York Academy of Sciences, 899,274-82. Retrieved from http://onlinelibrary.wiley.com/wol1/doi/10.1111/j.1749-6632.2000.tb06193.x/full. Heutink, M., Post, M.W., Wollaars, M.M., and van Asbeck, F.W. (2011). Chronic spinal cord injury pain: pharmacological and non-pharmacological treatments and treatment effectiveness. Disability and Rehabilitation, 33(5), 433-40. Retrieved from http://www.tandfonline.com/doi/full/10.3109/09638288.2010.498557?needAccess=true. Hussain, S.A., Zhou, R., Jacobson, C., Weng, J., Cheng, E., Lay, J., Hung, P., Lerner, J.T., and Sankar, R. (2015, June). Perceived efficacy of cannabidiol-enriched cannabis extracts for treatment of pediatric epilepsy: A potential role for infantile spasms and Lennox-Gastaut syndrome. Epilepsy & Behavior, 47, 138-41. Retrieved from http://www.epilepsybehavior.com/article/S1525-5050(15)00157-2/fulltext. Iuvone, T., Esposito, G., Esposito, R., Santamaria, R., Di Rosa, M., and Izzo, A.A. (2004, April). Neuroprotective effect of cannabidiol, a non-psychoactive component from Cannabis sativa, on beta-amyloid-induced toxicity in PC12 cells. Journal of Neurochemistry, 89(1), 134-41. Retrieved from http://onlinelibrary.wiley.com/doi/10.1111/j.1471-4159.2003.02327.x/full. Jensen, B., Chen, J., Furnish, T., and Wallace, M. (2015, October). Medical Marijuana and Chronic Pain: a Review of Basic Science and Clinical Evidence. Current Pain and Headache Reports, 19(10), 524. Retrieved from http://link.springer.com/article/10.1007%2Fs11916-015-0524-x. Jiang, W., Zhang, Y., Xiao, L., Van Cleemput, J., Ji, S.P., Bai, G., and Zhang, X. (2005). Cannabinoids promote embryonic and adult hippocampus neurogenesis and produce anxiolytic- and antidepressant-like effects. Journal of Clinical Investigation, 115(11), 3104–3116. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1253627/. Kim, S.H., Won, S.J., Mao, X.O., Jin, K., and Greenberg, D.A. (2006, March). Molecular mechanisms of cannabinoid protection from neuronal excitotoxicity. Molecular Pharmacology, 69(30), 691-6. Retrieved from http://molpharm.aspetjournals.org/content/69/3/691.long. Kubajewska, I., and Constantinescu, C.S. (2010, August). Cannabinoids and experimental models of multiple sclerosis. Immunobiology, 215(8), 647-57. Retrieved from http://www.sciencedirect.com/science/article/pii/S0171298509001442. Kwiatkoski, M., Guimaraes, F.S., and Del-Bel, E. (2012, April). Cannabidiol-treated rats exhibited higher motor score after cryogenic spinal cord injury. Neurotoxicity Research, 21(3), 271-80. Retrieved from http://link.springer.com/article/10.1007%2Fs12640-011-9273-8. Lafuente, H., Alvarez, F.J., Pazos, M.R., Alvarez, A., Rey-Santano, M.C., Mielgo, V., Murgia-Esteve, X., Hilario, E., and Martinez-Orgado, J. (2011, September). Cannabidiol reduces brain damage and improves functional recovery after acute hypoxia-ischemia in newborn pigs. Pediatric Research, 70(3), 272-7. Retrieved from http://www.nature.com/pr/journal/v70/n3/full/pr2011171a.html. Lastres-Becker, I., and Fernandez-Ruiz, J. (2006). An overview of Parkinson’s disease and the cannabinoid system and possible benefits of cannabinoid-based treatments. Current Medicinal Chemistry, 13(30< 3705-18. Retrieved from http://www.eurekaselect.com/58342/article. Latini, L., Bisicchia, E., Sasso, V., Chiurchiu, V., Cavallucci, V., Molinari, M., Maccarrone, M., and Viscomi, M.T. (2014, September 4). Cannabinoid CB2 receptor (CB2R). stimulation delays rubrospinal mitochondrial-dependent degeneration and improves functional recovery after spinal cord hemisection by ERK1/2 inactivation. Cell Death & Disease, e1404. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4540196/. López Rodríguez, A.B., Siopi, E., Finn, D.P., Marchand-Leroux, C., Garcia-Segura, L.M., Jafarian-Tehrani, M.H., and Viveros, M.P. (2013). CB1 and CB2 cannabinoid receptor antagonists prevent minocycline-induced neuroprotection following traumatic brain injury in mice. Cerebral Cortex. Retrieved from http://cercor.oxfordjournals.org/content/early/2013/08/19/cercor.bht202.abstract. Lotan, I., Treves, T., Roditi, Y., and Djaldetti, R. (2014, March/April). Cannabis (medical marijuana) treatment for motor and nonmotor symptoms of Parkinson disease: an open-label bbservational study. Clinical Neuropharmacology, 37(2), 41-44. Retrieved from http://journals.lww.com/clinicalneuropharm/pages/articleviewer.aspx?year=2014&issue=03000&article=00001&type=abstract. Marsicano, G., Goodenough, S., Monory, K., Hermann, H., Eder, M., Cannich, A., Azad, S.C., Cascio, M.G., Gutiérrez, S.O., van der Stelt, M., López-Rodriguez, M.L., Casanova, E., Schütz, G., Zieglgänsberger, W., Di Marzo, V., Behl, C., and Lutz, B. (2003, October 3). CB1 Cannabinoid Receptors and On-Demand Defense Against Excitotoxicity. Science, 302(5642), 84-8. Retrieved from http://science.sciencemag.org/content/302/5642/84/tab-pdf. Massi, P., Vaccani, A., Ceruti, S., Colombo, A. Abbracchio, M.P., and Parolaro, D. (2004, March). Antitumor effects of cannabidiol, a nonpsychoactive cannabinoid, on human glioma cell lines. The Journal of Pharmacology and Experimental Therapeutics, 308(3), 838-45. Retrieved from http://jpet.aspetjournals.org/content/308/3/838.long. McDonough, P., McKenna, J.P., McCreary, C., and Downer, E.J. (2014, October). Neuropathic orofacial pain: cannabinoids as a therapeutic avenue. The International Journal of Biochemistry & Cell Biology, 55, 72-8. Retrieved from http://www.sciencedirect.com/science/article/pii/S1357272514002581. Mechoulam, R., and Hanus, L. (2001). The cannabinoids: An overview. Therapeutic implications in vomiting and nausea after cancer chemotherapy, in appetite promotion, in multiple sclerosis and in neuroprotection. Pain Research and Management, 6(2), 67-73. Retrieved from http://downloads.hindawi.com/journals/prm/2001/183057.pdf. More, S.V., and Choi, D.K. (2015, April). Promising cannabinoid-based therapies for Parkinson’s disease: motor symptoms to neuroprotection. Molecular Neurodegeneration, 10, 17. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4404240/. Muller-Vahl, K.R., Schneider, U., Koblenz, A., Jobges, M., Kolbe, H., Daldrup, T., and Emrich, H.M. (2002, March). Treatment of Tourette’s syndrome with Delta 9-tetrahydrocannabinol (THC): a randomized crossover trial. Pharmacopsychiatry, 35(2), 57-61. Retrieved from https://www.thieme-connect.com/DOI/DOI?10.1055/s-2002-25028. Muller-Vahl, K.R. (2003). Cannabinoids reduce symptoms of Tourette’s syndrome. Expert Opinion on Pharmacotherapy, 4(10), 1717-1725. Retrieved from http://www.tandfonline.com/doi/pdf/10.1517/14656566.4.10.1717?needAccess=true. Muller-Vahl, K.R. (2013). Treatment of Tourette syndrome with cannabinoids. Behavioral Neurology, 27(1), 119-24. Retrieved from http://downloads.hindawi.com/journals/bn/2013/294264.pdf. Neurological Disorders. (n.d.). UCSF Medical Center. Retrieved from http://www.ucsfhealth.org/conditions/neurological_disorders/. Novotna, A., Mares, J., Ratcliffe, S., Novakova, I., Vachova, M., Zapletalova, O., Gasperini, C., Pozzilli, C., Cefaro, L., Comi, G., Rossi, P., Ambler, Z., Stelmasiak, Z., Erdmann, A., Montalban, X., Klimek, A., Davies, P. (2011, September). A randomized double-blind-placebo-controlled, parallel-group, enriched-design study of nabiximols* (Sativex(®), as add-on therapy, in subjects with refractory spasticity caused by multiple sclerosis. European Journal of Neurology, 18(9), 1122-31. Retrieved from http://onlinelibrary.wiley.com/wol1/doi/10.1111/j.1468-1331.2010.03328.x/full. Pope, C., Mechoulam, R., and Parsons, L. (2010). Endocannabinoid Signalling in Neurotoxicity and Neuroprotection. Neurotoxicology, 31(5), 562–571. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2891218/. Pryce, G., Ahmed, Z., Hankey, D.J., Jackson, S.J., Croxford, J.L. Pocock, J.M., Ledent, C., Petzold, A., Thompson, A.J., Giovannoni, G., Cuzner, M.L., and Baker, D. (2003, October). Cannabinoids inhibit neurodegeneration in models of multiple sclerosis. Brain, 126(Pt 10), 2191-202. Retrieved from https://academic.oup.com/brain/article-lookup/doi/10.1093/brain/awg224. Raman, C., McAllister, S.D., Rizvi, G., Patel, S.G., Moore, D.H., and Abood, M.E. (2004). Amyotrophic lateral sclerosis: delayed disease progression in mice by treatment with a cannabinoid. Amyotrophic Lateral Sclerosis & Other Motor Neuron Disorders, 5(1), 33-30. Retrieved from http://www.tandfonline.com/doi/abs/10.1080/14660820310016813. Rosenberg, E.C., Tsien, R.W, Whalley, B.J., and Devinsky, O. (2015, August 18). Cannabinoids and Epilepsy. Neurotherapeutics, Epub ahead of print. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/26282273. Sagredo, O., Garcia-Arencibia, M., de Lago, E., Finetti, S., Decio, A., and Fernandez-Ruiz, J. (2007, August). Cannabinoids and Neuroprotection in Basal Ganglia Disorders. Molecular Neurobiology, 36(1), 82-91. Retrieved from http://link.springer.com/article/10.1007%2Fs12035-007-0004-3. Scotter, E.L., Abood, M.E., and Glass, M. (2010). The endocannabinoid system as a target for the treatment of neurodegenerative disease. British Journal of Pharmacology, 160(3), 480–498. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2931550/. Szaflarski, J.P., and Bebin, E.M. (2014, December). Cannabis, cannabidiol, and epilepsy–from receptors to clinical response. Epilepsy & Behavior, 41, 277-82. Retrieved from http://www.epilepsybehavior.com/article/S1525-5050(14)00413-2/fulltext. van der Stelt, M., Veldhuis, W.B., Bar, P.R., Veldink, G.A., Vliegenthart, J.F., and Nicolay, K. (2001, September 1). Neuroprotection by Δ9-Tetrahydrocannabinol, the Main Active Compound in Marijuana, against Ouabain-Induced In Vivo Excitotoxicity. The Journal of Neuroscience, 21(17), 6475-9. Retrieved from http://www.jneurosci.org/content/21/17/6475.long. Weydt, P., Hong, S., Witting, A., Moller, T., Stella, N., and Kliot, M. (2005). Cannabinol delays symptom onset in SOD1 transgenic mice without affecting survival. Amyotrophic Lateral Sclerosis & Other Motor Neuron Disorders, 6(3), 182-184. Retrieved from http://www.tandfonline.com/doi/abs/10.1080/14660820510030149?journalCode=iafd19. Wilsey, B., Marcotte, T.D., Deutsch, R., Gouaux, B., Sakai, S., and Donaghe, H. (2003, February). Low dose vaporized cannabis significantly improves neuropathic pain. Journal of Pain, 14(2), 136-148. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3566631/. Witting, A., Chen, L., Cudaback, E., Straiker, A., Walter, L., Rickman, B., Moller, T., Brosnan, C., and Stella, N. (2006, April 18). Experimental autoimmune encephalomyelitis disrupts endocannabinoid-mediated neuroprotection. PNAS, 103(16), 6362-7. Retrieved from http://www.pnas.org/content/103/16/6362.full. Wolf, S.A., Bick-Sander, A., Fabel, K., Leal-Galicia, P., Tauber, S., Ramirez-Rodriguez, G., Muller, A., Melnik, A., Waltinger, T.P., Ullrich, O., and Kempermann, G. (2010). Cannabinoid receptor CB1 mediates baseline and activity-induced survival of new neurons in adult hippocampal neurogenesis. Cell Communication and Signaling : CCS, 8, 12. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2898685/. Zogopoulos, P., Vasileiou, I., Patsouris, E., and Theocharis, S. (2013, April). The neuroprotective role of endocannabinoids against chemical-induced injury and other adverse effects. Journal of Applied Toxicology, 33(4), 246-64. Retrieved from http://onlinelibrary.wiley.com/wol1/doi/10.1002/jat.2828/full. Zuardi, A.W. (2008, September). Cannabidiol: from an inactive cannabinoid to a drug with wide spectrum of action. Revista Brasileira De Psiquiatria, 30(3), 271-80. Retrieved from http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1516-44462008000300015&lng=en&nrm=iso&tlng=en.]]>
Appendix A:
WHEREAS cannabis (marijuana) has been used as a medicine for at least 5,000 years and can be effective for serious medical conditions for which conventional medications fail to provide relief;
WHEREAS modern medical research has shown that cannabis can slow the progression of such serious diseases as Alzheimer’s and Parkinson’s and stop HIV and cancer cells from spreading; has both anti-inflammatory and pain-relieving properties; can alleviate the symptoms of epilepsy, PTSD and multiple sclerosis; is useful in the treatment of depression, anxiety and other mental disorders; and can help reverse neurological damage from brain injuries and stroke;
WHEREAS the World Health Organization has acknowledged the therapeutic effects of cannabinoids, the primary active compounds found in cannabis, including as an anti-depressant, appetite stimulant, anticonvulsant and anti-spasmodic, and identified cannabinoids as beneficial in the treatment of asthma, glaucoma, and nausea and vomiting related to illnesses such as cancer and AIDS;
WHEREAS the American Medical Association has called for the review of the classification of cannabis as a Schedule I controlled substance to allow for clinical research and the development of cannabinoid-based medicines;
WHEREAS the National Cancer Institute has concluded that cannabis has antiemetic effects and is beneficial for appetite stimulation, pain relief, and improved sleep among cancer patients;
WHEREAS the American Herbal Pharmacopoeia and the American Herbal Products Association have developed qualitative standards for the use of cannabis as a botanical medicine;
WHEREAS the U.S. Supreme Court has long noted that states may operate as “laboratories of democracy” in the development of innovative public policies;
WHEREAS twenty-eight states and the District of Columbia have enacted laws that allow for the medical use of cannabis;
WHEREAS seventeen additional states have enacted laws authorizing the medical use of therapeutic compounds extracted from the cannabis plant;
WHEREAS more than 17 years of state-level experimentation provides a guide for state and federal law and policy related to the medical use of cannabis;
WHEREAS accredited educational curricula concerning the medical use of cannabis have been established that meets Continuing Medical Education requirements for practicing physicians;
WHEREAS Congress has prohibited the federal Department of Justice from using funds to interfere with and prosecute those acting in compliance with their state medical cannabis laws, and the Department of Justice has issued guidance to U.S. Attorneys indicating that enforcement of the Controlled Substances Act is not a priority when individual patients and their care providers are in compliance with state law, and that federal prosecutors should defer to state and local enforcement so long as a viable state regulatory scheme is in place;
WHEREAS modern medical research has shown that cannabis can slow the progression of such serious diseases as Alzheimer’s and Parkinson’s and stop HIV and cancer cells from spreading; has both anti-inflammatory and pain-relieving properties; can alleviate the symptoms of epilepsy, PTSD and multiple sclerosis; is useful in the treatment of depression, anxiety and other mental disorders; and can help reverse neurological damage from brain injuries and stroke;
WHEREAS the World Health Organization has acknowledged the therapeutic effects of cannabinoids, the primary active compounds found in cannabis, including as an anti-depressant, appetite stimulant, anticonvulsant and anti-spasmodic, and identified cannabinoids as beneficial in the treatment of asthma, glaucoma, and nausea and vomiting related to illnesses such as cancer and AIDS;
WHEREAS the American Medical Association has called for the review of the classification of cannabis as a Schedule I controlled substance to allow for clinical research and the development of cannabinoid-based medicines;
WHEREAS the National Cancer Institute has concluded that cannabis has antiemetic effects and is beneficial for appetite stimulation, pain relief, and improved sleep among cancer patients;
WHEREAS the American Herbal Pharmacopoeia and the American Herbal Products Association have developed qualitative standards for the use of cannabis as a botanical medicine;
WHEREAS the U.S. Supreme Court has long noted that states may operate as “laboratories of democracy” in the development of innovative public policies;
WHEREAS twenty-eight states and the District of Columbia have enacted laws that allow for the medical use of cannabis;
WHEREAS seventeen additional states have enacted laws authorizing the medical use of therapeutic compounds extracted from the cannabis plant;
WHEREAS more than 17 years of state-level experimentation provides a guide for state and federal law and policy related to the medical use of cannabis;
WHEREAS accredited educational curricula concerning the medical use of cannabis have been established that meets Continuing Medical Education requirements for practicing physicians;
WHEREAS Congress has prohibited the federal Department of Justice from using funds to interfere with and prosecute those acting in compliance with their state medical cannabis laws, and the Department of Justice has issued guidance to U.S. Attorneys indicating that enforcement of the Controlled Substances Act is not a priority when individual patients and their care providers are in compliance with state law, and that federal prosecutors should defer to state and local enforcement so long as a viable state regulatory scheme is in place;
No comments:
Post a Comment